

Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection
- PMID: 33631096
- PMCID: PMC7871851
- DOI: 10.1016/j.cell.2021.02.010
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection
Abstract
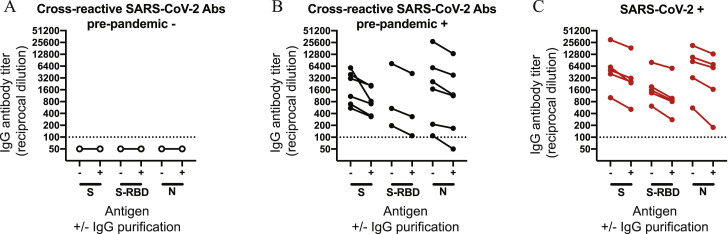
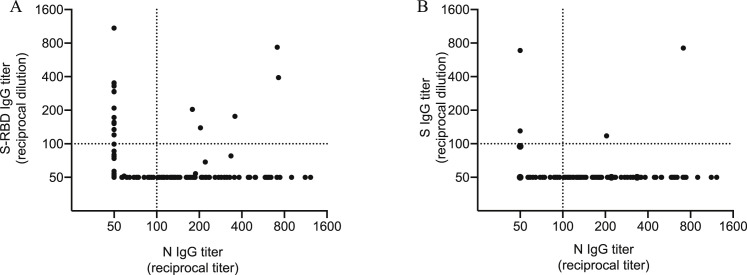
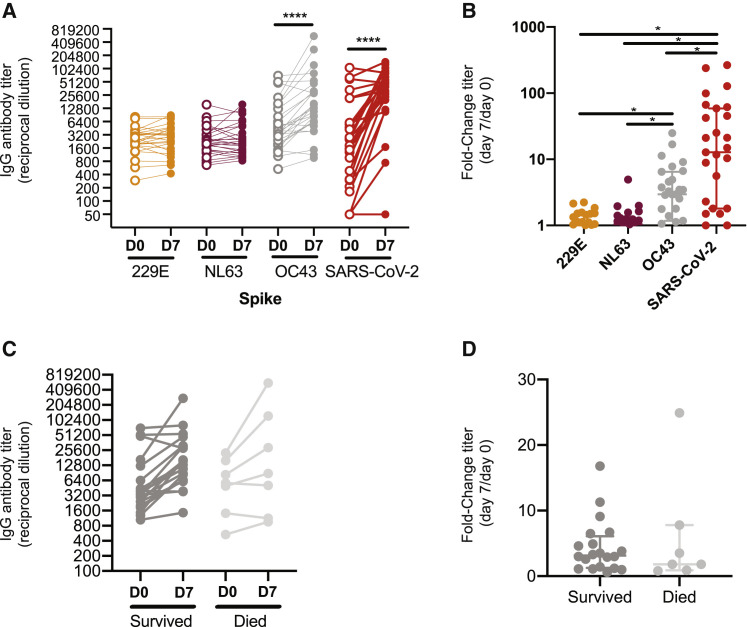
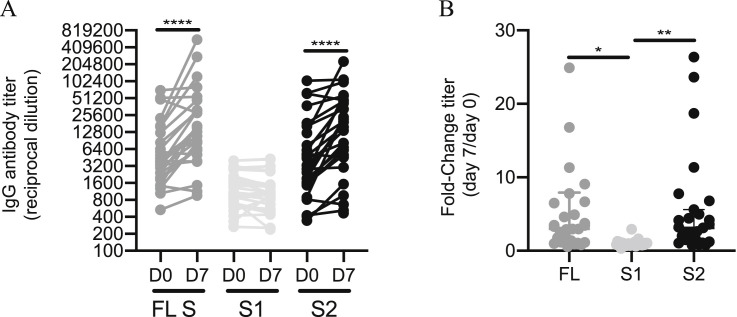
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly spread within the human population. Although SARS-CoV-2 is a novel coronavirus, most humans had been previously exposed to other antigenically distinct common seasonal human coronaviruses (hCoVs) before the coronavirus disease 2019 (COVID-19) pandemic. Here, we quantified levels of SARS-CoV-2-reactive antibodies and hCoV-reactive antibodies in serum samples collected from 431 humans before the COVID-19 pandemic. We then quantified pre-pandemic antibody levels in serum from a separate cohort of 251 individuals who became PCR-confirmed infected with SARS-CoV-2. Finally, we longitudinally measured hCoV and SARS-CoV-2 antibodies in the serum of hospitalized COVID-19 patients. Our studies indicate that most individuals possessed hCoV-reactive antibodies before the COVID-19 pandemic. We determined that ∼20% of these individuals possessed non-neutralizing antibodies that cross-reacted with SARS-CoV-2 spike and nucleocapsid proteins. These antibodies were not associated with protection against SARS-CoV-2 infections or hospitalizations, but they were boosted upon SARS-CoV-2 infection.
Keywords: SARS-CoV-2; antibodies; coronavirus; pre-existing immunity.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.C.H. is a consultant for Immunai. E.J.W. has consulting agreements with and/or is on the scientific advisory board for Merck, Elstar, Janssen, Related Sciences, Synthekine, and Surface Oncology. E.J.W. is a founder of Surface Oncology and Arsenal Biosciences. E.J.W. is an inventor on a patent (U.S. patent number 10,370,446) submitted by Emory University that covers the use of PD-1 blockade to treat infections and cancer. D.J.R. is on scientific advisory boards for Alnylam, Metrea, Novartis, Pfizer, and Verve; is a consultant for and receives research support from Regeneron for work unrelated to this report; and is a founder of Vascular Strategies and Staten Biotechnologies. S.E.H. has received consultancy fee from Sanofi Pasteur, Lumen, Novavax, and Merck for work unrelated to this report.
Figures






Update of
-
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection.medRxiv [Preprint]. 2020 Nov 10:2020.11.06.20227215. doi: 10.1101/2020.11.06.20227215. medRxiv. 2020. Update in: Cell. 2021 Apr 1;184(7):1858-1864.e10. doi: 10.1016/j.cell.2021.02.010 PMID: 33200143 Free PMC article. Updated. Preprint.
Similar articles
-
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection.medRxiv [Preprint]. 2020 Nov 10:2020.11.06.20227215. doi: 10.1101/2020.11.06.20227215. medRxiv. 2020. Update in: Cell. 2021 Apr 1;184(7):1858-1864.e10. doi: 10.1016/j.cell.2021.02.010 PMID: 33200143 Free PMC article. Updated. Preprint.
-
Cross-Reactive Antibodies to SARS-CoV-2 and MERS-CoV in Pre-COVID-19 Blood Samples from Sierra Leoneans.Viruses. 2021 Nov 21;13(11):2325. doi: 10.3390/v13112325. Viruses. 2021. PMID: 34835131 Free PMC article.
-
Detection of Serum Cross-Reactive Antibodies and Memory Response to SARS-CoV-2 in Prepandemic and Post-COVID-19 Convalescent Samples.J Infect Dis. 2021 Oct 28;224(8):1305-1315. doi: 10.1093/infdis/jiab333. J Infect Dis. 2021. PMID: 34161567 Free PMC article.
-
Antibody Mediated Immunity to SARS-CoV-2 and Human Coronaviruses: Multiplex Beads Assay and Volumetric Absorptive Microsampling to Generate Immune Repertoire Cartography.Front Immunol. 2021 Jul 27;12:696370. doi: 10.3389/fimmu.2021.696370. eCollection 2021. Front Immunol. 2021. PMID: 34386006 Free PMC article.
-
Cross-Reactive Immune Responses toward the Common Cold Human Coronaviruses and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Mini-Review and a Murine Study.Microorganisms. 2021 Jul 31;9(8):1643. doi: 10.3390/microorganisms9081643. Microorganisms. 2021. PMID: 34442723 Free PMC article. Review.
Cited by
-
Cas12a-assisted RTF-EXPAR for accurate, rapid and simple detection of SARS-CoV-2 RNA.Biosens Bioelectron. 2022 Nov 15;216:114683. doi: 10.1016/j.bios.2022.114683. Epub 2022 Sep 6. Biosens Bioelectron. 2022. PMID: 36088673 Free PMC article.
-
Humoral cross-coronavirus responses against the S2 region in children with Kawasaki disease.Virology. 2022 Oct;575:83-90. doi: 10.1016/j.virol.2022.08.010. Epub 2022 Sep 2. Virology. 2022. PMID: 36088793 Free PMC article.
-
Studying the Humoral Response against SARS-CoV-2 in Cuban COVID-19 Recovered Patients.J Immunol Res. 2024 Sep 25;2024:7112940. doi: 10.1155/2024/7112940. eCollection 2024. J Immunol Res. 2024. PMID: 39359695 Free PMC article.
-
Development and Validation of a Highly Sensitive Multiplex Immunoassay for SARS-CoV-2 Humoral Response Monitorization: A Study of the Antibody Response in COVID-19 Patients with Different Clinical Profiles during the First and Second Waves in Cadiz, Spain.Microorganisms. 2023 Dec 16;11(12):2997. doi: 10.3390/microorganisms11122997. Microorganisms. 2023. PMID: 38138141 Free PMC article.
-
Immune Responses to COVID-19 mRNA Vaccines in Patients with Solid Tumors on Active, Immunosuppressive Cancer Therapy.medRxiv [Preprint]. 2021 Aug 25:2021.05.13.21257129. doi: 10.1101/2021.05.13.21257129. medRxiv. 2021. Update in: Nat Med. 2021 Nov;27(11):2002-2011. doi: 10.1038/s41591-021-01542-z PMID: 34013289 Free PMC article. Updated. Preprint.
References
-
- Braun J., Loyal L., Frentsch M., Wendisch D., Georg P., Kurth F., Hippenstiel S., Dingeldey M., Kruse B., Fauchere F., et al. SARS-CoV-2-reactive T cells in healthy donors and patients with COVID-19. Nature. 2020;587:270–274. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
