

Liver cancer mortality over six decades in an epidemic area: what we have learned
- PMID: 33604165
- PMCID: PMC7866902
- DOI: 10.7717/peerj.10600
Liver cancer mortality over six decades in an epidemic area: what we have learned
Abstract
Background and aims: Liver cancer is one of the most dominant malignant tumors in the world. The trends of liver cancer mortality over the past six decades have been tracked in the epidemic region of Qidong, China. Using epidemiological tools, we explore the dynamic changes in age-standardized rates to characterize important aspects of liver cancer etiology and prevention.
Methods: Mortality data of liver cancer in Qidong from 1958 to 1971 (death retrospective survey) and from 1972 to 2017 (cancer registration) were tabulated for the crude rate (CR), and age-standardized rate and age-birth cohorts. The average annual percentage change was calculated by the Joinpoint Regression Program.
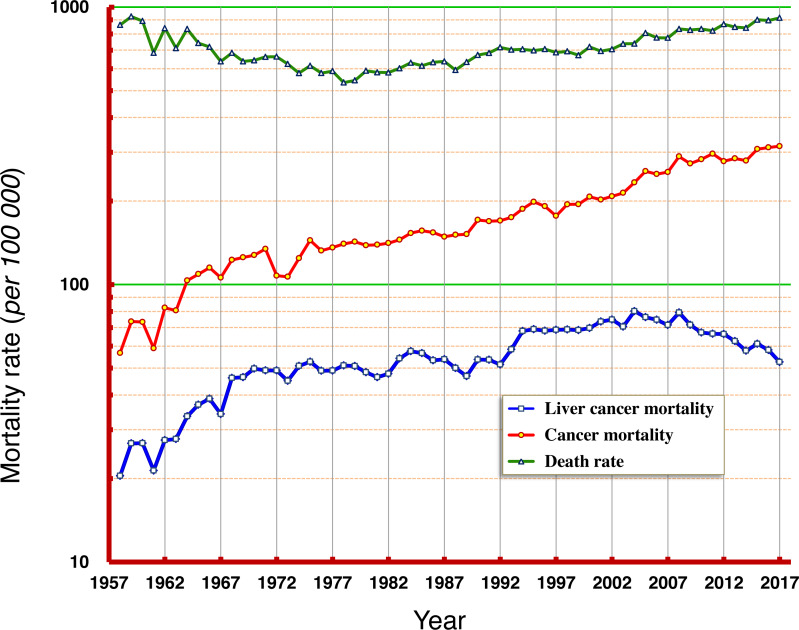
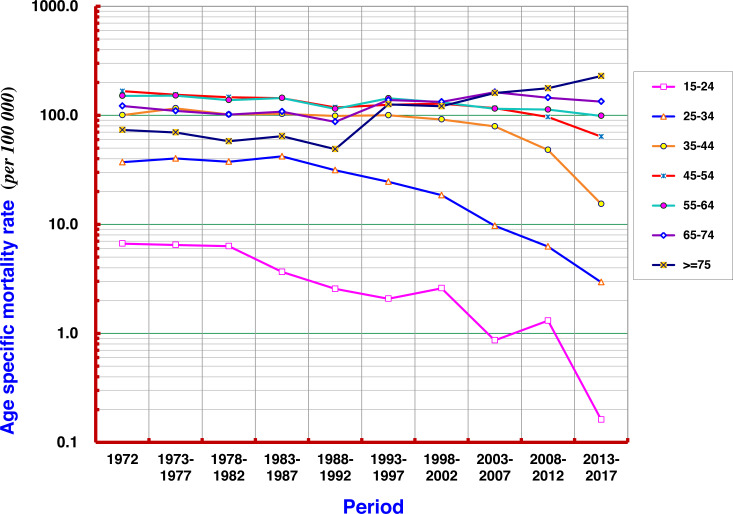
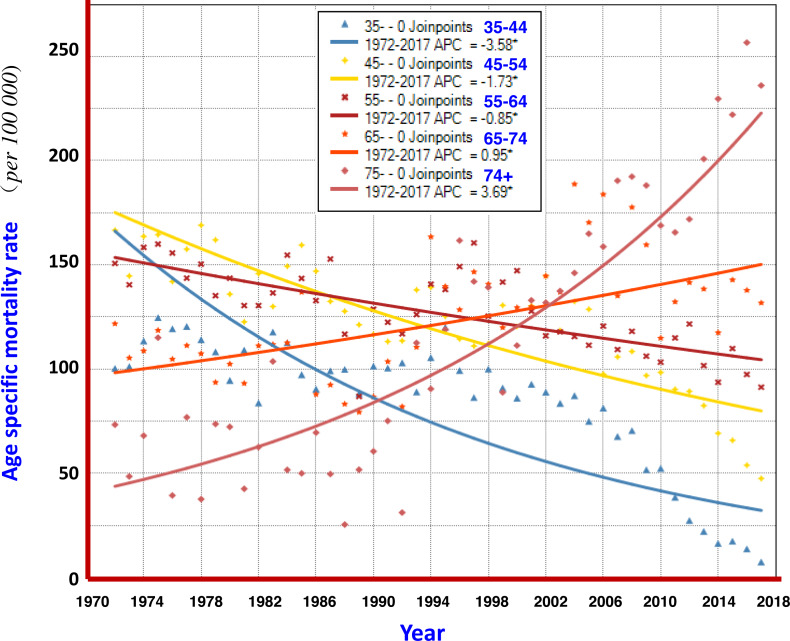
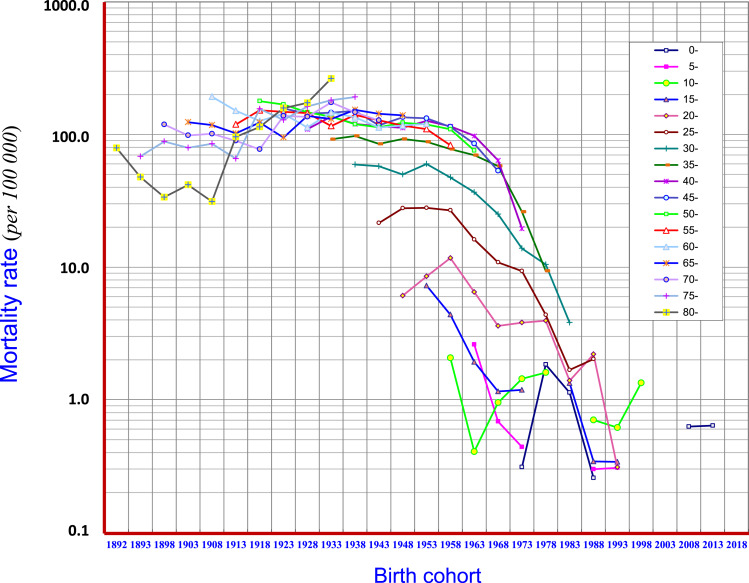
Results: The natural death rate during 1958-2017 decreased from 9‰ to 5.4‰ and then increased to 8‰ as the population aged; cancer mortality rates rose continuously from 57/105 to 240/105. Liver cancer mortality increased from 20/105 to 80/105, and then dropped to less than 52/105 in 2017. Liver cancer deaths in 1972-2017 accounted for 30.53% of all cancers, with a CR of 60.48/105, age-standardized rate China (ASRC) of 34.78/105, and ASRW (world) of 45.71/105. Other key features were the CR for males and females of 91.86/105 and 29.92/105, respectively, with a sex ratio of 3.07:1. Period analysis showed that the ASRs for mortality of the age groups under 54 years old had a significant decreasing trend. Importantly, birth cohort analysis showed that the mortality rate of liver cancer in 40-44, 35-39, 30-34, 25-29, 20-24, 15-19 years cohort decreased considerably, but the rates in 70-74, and 75+ increased.
Conclusions: The crude mortality rate of liver cancer in Qidong has experienced trends from lower to higher levels, and from continued increase at a high plateau to most recently a gradual decline, and a change greatest in younger people. Many years of comprehensive prevention and intervention measures have influenced the decline of the liver cancer epidemic in this area. The reduction of intake levels of aflatoxin might be one of the most significant factors as evidenced by the dramatic decline of exposure biomarkers in this population during the past three decades.
Keywords: Age-standardized rate; Annual percentage change; Birth cohort; Epidemiology; Liver cancer; Mortality; Trend.
©2021 Chen et al.
Conflict of interest statement
The authors declare there are no competing interests.
Figures
 ), females (
), females (  ) and both sexes (
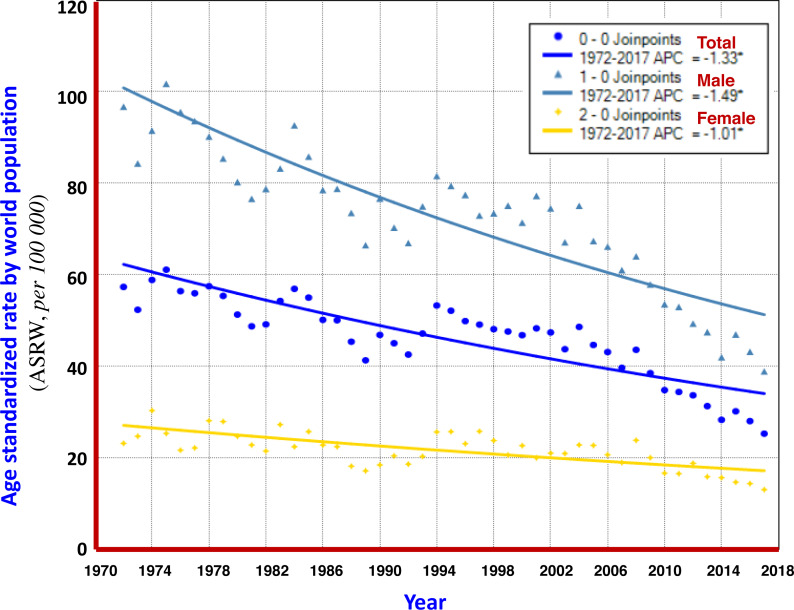
) and both sexes (  ). The Joinpoint Regression analysis shows that AAPCs of ASRW were −1.49% for men (
). The Joinpoint Regression analysis shows that AAPCs of ASRW were −1.49% for men (  ), −1.01% for women (
), −1.01% for women (  ), and −1.33% for both sexes (
), and −1.33% for both sexes (  ).
).
 ), females (
), females (  ) and both sexes (
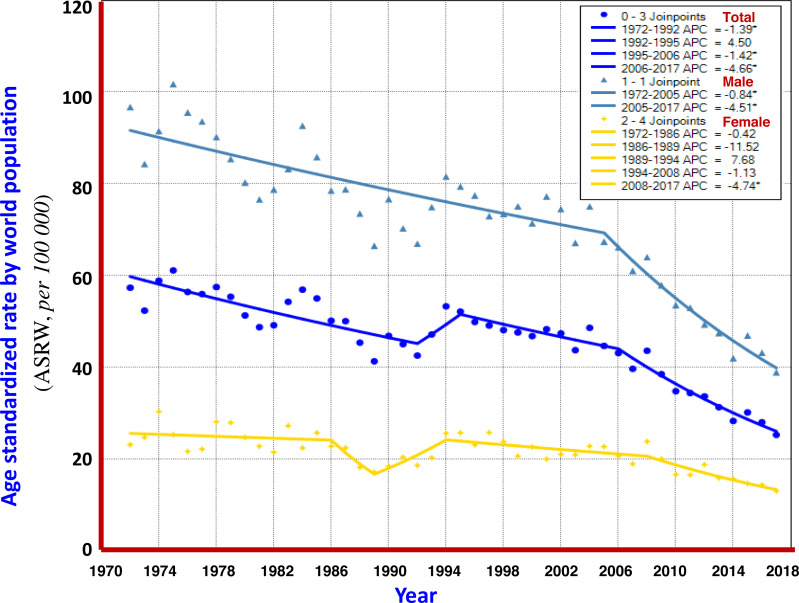
) and both sexes (  ). Turning point analysis of multiple models shows that the trend in ASRW of liver cancer during the period could be divided into three joinpoints (four periods) for both sexes (
). Turning point analysis of multiple models shows that the trend in ASRW of liver cancer during the period could be divided into three joinpoints (four periods) for both sexes (  ). For men, it was one point (2 periods,
). For men, it was one point (2 periods,  ), and for women, four joinpoints (5 periods,
), and for women, four joinpoints (5 periods,  ).
).
 ), men (
), men (  ), and women (
), and women (  ).
).
Similar articles
-
[Trends in the mortality of liver cancer in Qidong, China: an analysis of fifty years].Zhonghua Zhong Liu Za Zhi. 2012 Jul;34(7):532-7. doi: 10.3760/cma.j.issn.0253-3766.2012.07.012. Zhonghua Zhong Liu Za Zhi. 2012. PMID: 22967473 Chinese.
-
[Trends and age-period-cohort analysis of leukemia incidence in Qidong from 1972 to 2021].Zhonghua Zhong Liu Za Zhi. 2024 Oct 23;46(10):961-967. doi: 10.3760/cma.j.cn112152-20240201-00061. Zhonghua Zhong Liu Za Zhi. 2024. PMID: 39414597 Chinese.
-
[Epidemic characteristics of esophageal cancer mortality in Qidong, 1972-2016].Zhonghua Zhong Liu Za Zhi. 2022 Oct 23;44(10):1096-1101. doi: 10.3760/cma.j.cn112152-20200225-00125. Zhonghua Zhong Liu Za Zhi. 2022. PMID: 36319455 Chinese.
-
Annual summary of vital statistics--1995.Pediatrics. 1996 Dec;98(6 Pt 1):1007-19. Pediatrics. 1996. PMID: 8951248 Review.
-
[Mortality Atlas of the Campania Region. All-cause and cause-specific mortality at municipal level, 2006-2014].Epidemiol Prev. 2020 Jan-Feb;44(1 Suppl 1):1-144. doi: 10.19191/EP20.1.S1.P001.003. Epidemiol Prev. 2020. PMID: 33565290 Review. Italian.
Cited by
-
ADH4-a potential prognostic marker for hepatocellular carcinoma with possible immune-related implications.BMC Cancer. 2024 Aug 1;24(1):927. doi: 10.1186/s12885-024-12675-y. BMC Cancer. 2024. PMID: 39090641 Free PMC article.
-
International comparison of trends in cancer mortality: Japan has fallen behind in screening-related cancers.Jpn J Clin Oncol. 2021 Nov 1;51(11):1680-1686. doi: 10.1093/jjco/hyab139. Jpn J Clin Oncol. 2021. PMID: 34467393 Free PMC article.
-
Global pattern of trends in incidence, mortality, and mortality-to-incidence ratio rates related to liver cancer, 1990-2019: a longitudinal analysis based on the global burden of disease study.BMC Public Health. 2022 Mar 29;22(1):604. doi: 10.1186/s12889-022-12867-w. BMC Public Health. 2022. PMID: 35351047 Free PMC article.
-
A Bibliometric Analysis of the Role of 3D Technology in Liver Cancer Resection.World J Surg. 2023 Jun;47(6):1548-1561. doi: 10.1007/s00268-023-06950-5. Epub 2023 Mar 7. World J Surg. 2023. PMID: 36882637 Review.
-
Liver Cancer Survival: A Real World Observation of 45 Years with 32,556 Cases.J Hepatocell Carcinoma. 2021 Aug 31;8:1023-1034. doi: 10.2147/JHC.S321346. eCollection 2021. J Hepatocell Carcinoma. 2021. PMID: 34513745 Free PMC article.
References
-
- Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, Bonaventure A, Valkov M, Johnson CJ, Estève J, Ogunbiyi OJ, Azevedo e Silva G, Chen WQ, Eser S, Engholm G, Stiller CA, Monnereau A, Woods RR, Visser O, Lim GH, Aitken J, Weir HK, Coleman MP, CONCORD Working Group Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. The Lancet. 2018;391(10125):1023–1075. doi: 10.1016/S0140-6736(17)33326-3. - DOI - PMC - PubMed
-
- Bray F, Colombet M, Mery L, Piñeros M, Znaor A, Zanetti R. Lyon: International Agency for Research on Cancer; 2020. [21 March 2020].
-
- Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, Liang DC, Shau WY, Chen DS. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. New England Journal of Medicine. 1997;336(26):1855–1859. doi: 10.1056/NEJM199706263362602. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
