

The Lymph Node Reservoir: Physiology, HIV Infection, and Antiretroviral Therapy
- PMID: 33529355
- PMCID: PMC8005487
- DOI: 10.1002/cpt.2186
The Lymph Node Reservoir: Physiology, HIV Infection, and Antiretroviral Therapy
Abstract
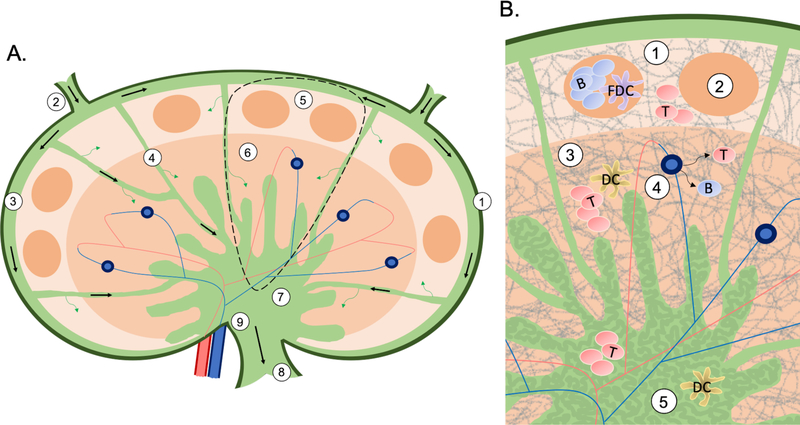
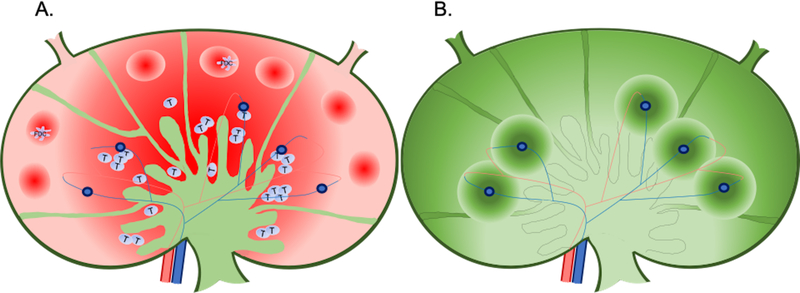
Despite advances in treatment, finding a cure for HIV remains a top priority. Chronic HIV infection is associated with increased risk of comorbidities, such as diabetes and cardiovascular disease. Additionally, people living with HIV must remain adherent to daily antiretroviral therapy, because lapses in medication adherence can lead to viral rebound and disease progression. Viral recrudescence occurs from cellular reservoirs in lymphoid tissues. In particular, lymph nodes are central to the pathology of HIV due to their unique architecture and compartmentalization of immune cells. Understanding how antiretrovirals (ARVs) penetrate lymph nodes may explain why these tissues are maintained as HIV reservoirs, and how they contribute to viral rebound upon treatment interruption. In this report, we review (i) the physiology of the lymph nodes and their function as part of the immune and lymphatic systems, (ii) the pathogenesis and outcomes of HIV infection in lymph nodes, and (iii) ARV concentrations and distribution in lymph nodes, and the relationship between ARVs and HIV in this important reservoir.
© 2021 The Authors Clinical Pharmacology & Therapeutics © 2021 American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
Conflict of Interest statement: All authors declared no competing interests for this work.
Figures
Similar articles
-
Quantitative Imaging Analysis of the Spatial Relationship between Antiretrovirals, Reverse Transcriptase Simian-Human Immunodeficiency Virus RNA, and Collagen in the Mesenteric Lymph Nodes of Nonhuman Primates.Antimicrob Agents Chemother. 2021 May 18;65(6):e00019-21. doi: 10.1128/AAC.00019-21. Print 2021 May 18. Antimicrob Agents Chemother. 2021. PMID: 33782003 Free PMC article.
-
Increased Proviral DNA in Circulating Cells Correlates with Plasma Viral Rebound in Simian Immunodeficiency Virus-Infected Rhesus Macaques after Antiretroviral Therapy Interruption.J Virol. 2021 Feb 24;95(6):e02064-20. doi: 10.1128/JVI.02064-20. Print 2021 Feb 24. J Virol. 2021. PMID: 33408173 Free PMC article.
-
Antiretroviral Drug Concentrations in Lymph Nodes: A Cross-Species Comparison of the Effect of Drug Transporter Expression, Viral Infection, and Sex in Humanized Mice, Nonhuman Primates, and Humans.J Pharmacol Exp Ther. 2019 Sep;370(3):360-368. doi: 10.1124/jpet.119.259150. Epub 2019 Jun 24. J Pharmacol Exp Ther. 2019. PMID: 31235531 Free PMC article.
-
The Contributions of Clinical Pharmacology to HIV Cure Research.Clin Pharmacol Ther. 2021 Aug;110(2):334-345. doi: 10.1002/cpt.2237. Epub 2021 Apr 18. Clin Pharmacol Ther. 2021. PMID: 33763860 Free PMC article. Review.
-
Is the Central Nervous System Reservoir a Hurdle for an HIV Cure?Viruses. 2023 Dec 5;15(12):2385. doi: 10.3390/v15122385. Viruses. 2023. PMID: 38140626 Free PMC article. Review.
Cited by
-
The Application of Prodrugs as a Tool to Enhance the Properties of Nucleoside Reverse Transcriptase Inhibitors.Viruses. 2023 Nov 9;15(11):2234. doi: 10.3390/v15112234. Viruses. 2023. PMID: 38005911 Free PMC article. Review.
-
Hybrid Lymphatic Drug Delivery Vehicles as a New Avenue for Targeted Therapy: Lymphatic Trafficking, Applications, Challenges, and Future Horizons.J Membr Biol. 2023 Jun;256(3):199-222. doi: 10.1007/s00232-023-00280-2. Epub 2023 Feb 8. J Membr Biol. 2023. PMID: 36752839 Free PMC article. Review.
-
Lymphoid tissues contribute to plasma viral clonotypes early after antiretroviral therapy interruption in SIV-infected rhesus macaques.Sci Transl Med. 2023 Dec 13;15(726):eadi9867. doi: 10.1126/scitranslmed.adi9867. Epub 2023 Dec 13. Sci Transl Med. 2023. PMID: 38091409 Free PMC article.
-
Controversies in the Design of Strategies for the Cure of HIV Infection.Pathogens. 2023 Feb 15;12(2):322. doi: 10.3390/pathogens12020322. Pathogens. 2023. PMID: 36839593 Free PMC article. Review.
-
Viral dissemination and immune activation modulate antiretroviral drug levels in lymph nodes of SIV-infected rhesus macaques.Front Immunol. 2023 Sep 18;14:1213455. doi: 10.3389/fimmu.2023.1213455. eCollection 2023. Front Immunol. 2023. PMID: 37790938 Free PMC article.
References
-
- Cihlar T & Fordyce M Current status and prospects of HIV treatment. Curr Opin Virol 18, 50–56 (2016). - PubMed
-
- Guaraldi G et al. Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin. Infect. Dis. 53, 1120–1126 (2011). - PubMed
-
- Duffau P et al. Multimorbidity, age-related comorbidities and mortality: association of activation, senescence and inflammation markers in HIV adults. AIDS 32, 1651–1660 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
