

Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study
- PMID: 33211135
- PMCID: PMC7674575
- DOI: 10.1007/s00134-020-06294-x
Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study
Abstract
Purpose: To describe acute respiratory distress syndrome (ARDS) severity, ventilation management, and the outcomes of ICU patients with laboratory-confirmed COVID-19 and to determine risk factors of 90-day mortality post-ICU admission.
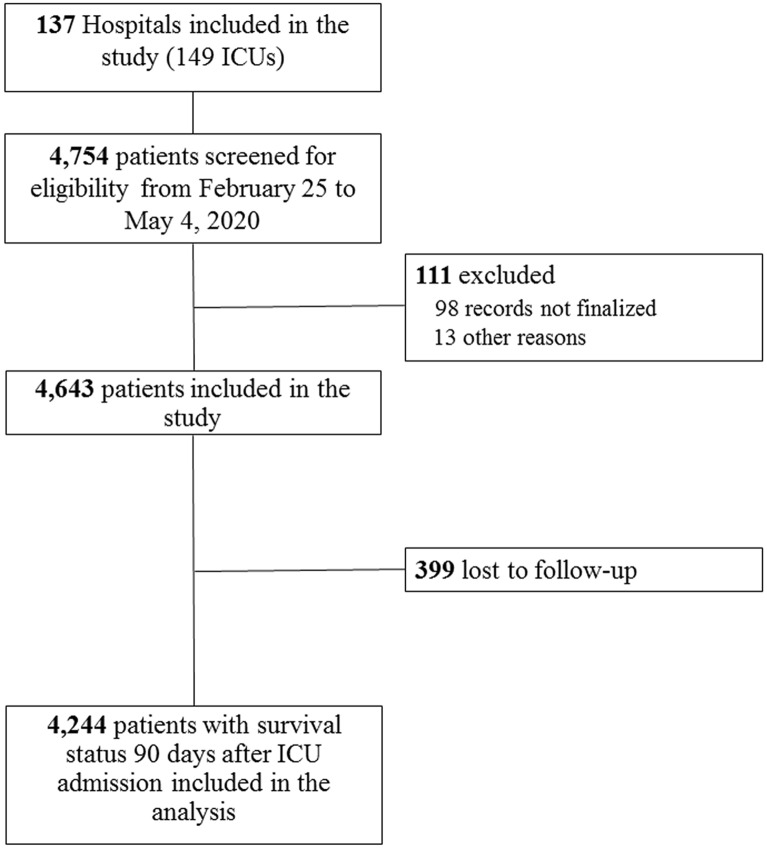
Methods: COVID-ICU is a multi-center, prospective cohort study conducted in 138 hospitals in France, Belgium, and Switzerland. Demographic, clinical, respiratory support, adjunctive interventions, ICU length-of-stay, and survival data were collected.
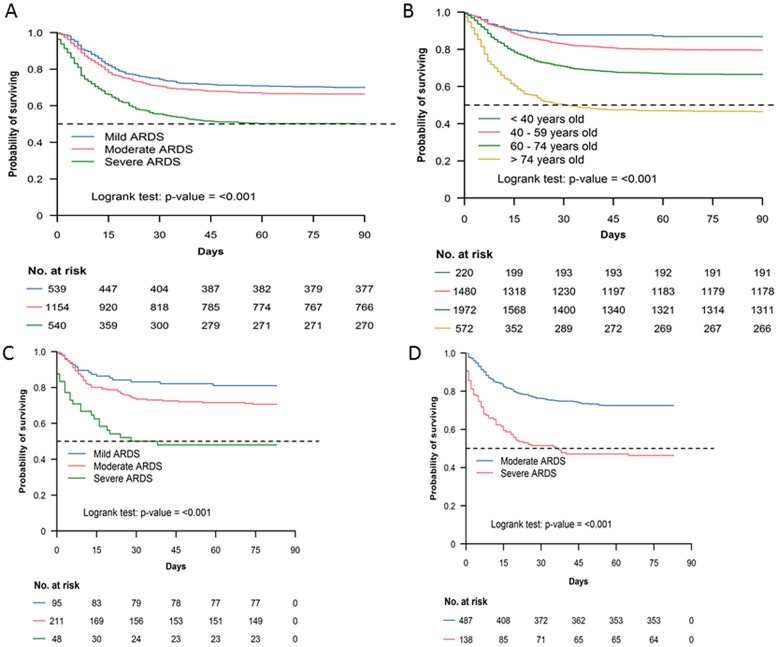
Results: From February 25 to May 4, 2020, 4643 patients (median [IQR] age 63 [54-71] years and SAPS II 37 [28-50]) were admitted in ICU, with day-90 post-ICU admission status available for 4244. On ICU admission, standard oxygen therapy, high-flow oxygen, and non-invasive ventilation were applied to 29%, 19%, and 6% patients, respectively. 2635 (63%) patients were intubated during the first 24 h whereas overall 3376 (80%) received invasive mechanical ventilation (MV) at one point during their ICU stay. Median (IQR) positive end-expiratory and plateau pressures were 12 (10-14) cmH2O, and 24 (21-27) cmH2O, respectively. The mechanical power transmitted by the MV to the lung was 26.5 (18.6-34.9) J/min. Paralyzing agents and prone position were applied to 88% and 70% of patients intubated at Day-1, respectively. Pulmonary embolism and ventilator-associated pneumonia were diagnosed in 207 (9%) and 1209 (58%) of these patients. On day 90, 1298/4244 (31%) patients had died. Among patients who received invasive or non-invasive ventilation on the day of ICU admission, day-90 mortality increased with the severity of ARDS at ICU admission (30%, 34%, and 50% for mild, moderate, and severe ARDS, respectively) and decreased from 42 to 25% over the study period. Early independent predictors of 90-day mortality were older age, immunosuppression, severe obesity, diabetes, higher renal and cardiovascular SOFA score components, lower PaO2/FiO2 ratio and a shorter time between first symptoms and ICU admission.
Conclusion: Among more than 4000 critically ill patients with COVID-19 admitted to our ICUs, 90-day mortality was 31% and decreased from 42 to 25% over the study period. Mortality was higher in older, diabetic, obese and severe ARDS patients.
Keywords: Acute respiratory distress syndrome; COVID-19; Mechanical ventilation; Mortality risk factor; Outcome.
Conflict of interest statement
MS reported personal fees from Getinge, Drager, and Xenios, outside the submitted work. AD reports personal fees from Medtronic, grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees from Hamilton, personal fees and non-financial support from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, grants and personal fees from Respinor, grants and non-financial support from Lungpacer, outside the submitted work. AM reported personal fees from Faron Pharmaceuticals, Air Liquid Medical Systems, Pfizer, Resmed and Draeger and grants and personal fees from Fisher and Paykel and Covidien, outside this work. MD reported personal fees from Lungpacer. AK reported personal fees from Aspen, Aguettant and MSD. No other disclosures were reported.
Figures
Similar articles
-
Clinical characteristics and outcomes of invasively ventilated patients with COVID-19 in Argentina (SATICOVID): a prospective, multicentre cohort study.Lancet Respir Med. 2021 Sep;9(9):989-998. doi: 10.1016/S2213-2600(21)00229-0. Epub 2021 Jul 2. Lancet Respir Med. 2021. PMID: 34224674 Free PMC article.
-
Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy.JAMA. 2020 Apr 28;323(16):1574-1581. doi: 10.1001/jama.2020.5394. JAMA. 2020. PMID: 32250385 Free PMC article.
-
SARS-CoV-2 in Spanish Intensive Care Units: Early experience with 15-day survival in Vitoria.Anaesth Crit Care Pain Med. 2020 Oct;39(5):553-561. doi: 10.1016/j.accpm.2020.04.001. Epub 2020 Apr 9. Anaesth Crit Care Pain Med. 2020. PMID: 32278670 Free PMC article.
-
Mechanical ventilation parameters in critically ill COVID-19 patients: a scoping review.Crit Care. 2021 Mar 20;25(1):115. doi: 10.1186/s13054-021-03536-2. Crit Care. 2021. PMID: 33743812 Free PMC article. Review.
-
Airway Pressure Release Ventilation in COVID-19-Associated Acute Respiratory Distress Syndrome-A Multicenter Propensity Score-Matched Analysis.J Intensive Care Med. 2024 Jan;39(1):84-93. doi: 10.1177/08850666231207303. Epub 2023 Oct 20. J Intensive Care Med. 2024. PMID: 37861125 Review.
Cited by
-
Extracorporeal Membrane Oxygenation instead of Invasive Mechanical Ventilation in a Patient with Severe COVID-19-associated Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2021 Jun 15;203(12):1571-1573. doi: 10.1164/rccm.202102-0259LE. Am J Respir Crit Care Med. 2021. PMID: 33901416 Free PMC article. No abstract available.
-
Ventilatory Management of Patients with Acute Respiratory Distress Syndrome Due to SARS-CoV-2.J Clin Med. 2023 Dec 5;12(24):7509. doi: 10.3390/jcm12247509. J Clin Med. 2023. PMID: 38137578 Free PMC article. Review.
-
Efficacy of umbilical cord mesenchymal stromal cells for COVID-19: A systematic review and meta-analysis.Front Immunol. 2022 Aug 29;13:923286. doi: 10.3389/fimmu.2022.923286. eCollection 2022. Front Immunol. 2022. PMID: 36105796 Free PMC article.
-
Respiratory system mechanics, gas exchange, and outcomes in mechanically ventilated patients with COVID-19-related acute respiratory distress syndrome: a systematic review and meta-analysis.Lancet Respir Med. 2022 Dec;10(12):1178-1188. doi: 10.1016/S2213-2600(22)00393-9. Epub 2022 Nov 3. Lancet Respir Med. 2022. PMID: 36335956 Free PMC article. Review.
-
Macrophage Migration Inhibitory Factor (MIF) Plasma Concentration in Critically Ill COVID-19 Patients: A Prospective Observational Study.Diagnostics (Basel). 2021 Feb 17;11(2):332. doi: 10.3390/diagnostics11020332. Diagnostics (Basel). 2021. PMID: 33671433 Free PMC article.
References
-
- REVA network http://www.reseau-reva.org/. Accessed 5 Oct 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
