

Clinical course of 602 patients with Takayasu's arteritis: comparison between Childhood-onset versus adult onset disease
- PMID: 33179052
- PMCID: PMC8599811
- DOI: 10.1093/rheumatology/keaa569
Clinical course of 602 patients with Takayasu's arteritis: comparison between Childhood-onset versus adult onset disease
Abstract
Objectives: To describe the clinical profile of Asian Indian patients with Takayasu's arteritis (TAK) and to compare clinical features and outcome of childhood-onset Takayasu's arteritis (cTAK) with adult-onset TAK (aTAK).
Methods: Data related to clinical features and response to treatment of patients with cTAK (age of onset <16 years) and aTAK from a large observational cohort in our tertiary care teaching hospital were noted and compared.
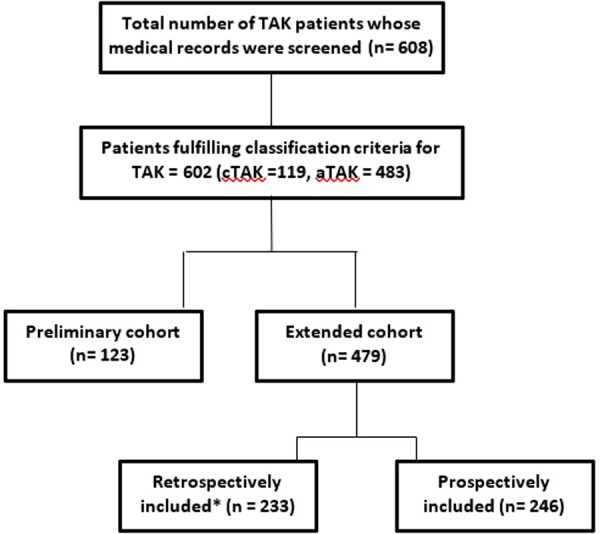
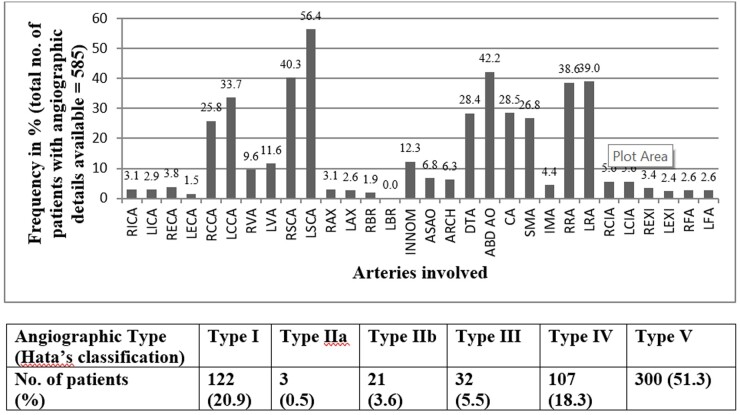
Results: Altogether, 602 patients (cTAK = 119; aTAK = 483) were studied. Patients with cTAK had a blunted female: male ratio; but fever, elevated acute phase reactants, involvement of abdominal aorta or its branches, hypertension, abdominal pain, elevated serum creatinine and cardiomyopathy were more common in cTAK as compared with aTAK. Patients with aTAK were more likely to have aortic-arch disease and claudication than cTAK. During follow-up, complete remission was more common in cTAK (87% vs 66%; P < 0.01), but subsequent relapses were equally common (30% vs 27%; P = 0.63). Independent associations of disease duration at presentation with disease extent [Disease Extent Index in TAK (DEI.Tak)] and damage [TAK Damage Score (TADS)] were observed (P ≤ 0.01). Moreover, 54% of patients with symptom duration of >5 years at presentation still continued to have elevated CRP suggesting continued and active inflammation warranting escalation or inititation of immunosuppression.
Conclusion: Patients with cTAK are more likely to have arterial disease below the diaphragm, systemic inflammation and achieve remission. Disease of the aortic arch is more common in patients with aTAK. Longer duration of symptoms prior to initiation of immunosuppression, thereby leading to extensive disease and damage, reflects ongoing disease activity as the rule rather than exception in untreated TAK.
Keywords: India; Takayasu’s arteritis; autoimmune; childhood Takayasu’s arteritis; childhood vasculitis; large-vessel vasculitis; vasculitis.
© The Author(s) 2020. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Is Takayasu's arteritis more severe in children?Clin Exp Rheumatol. 2021 Mar-Apr;39 Suppl 129(2):32-38. doi: 10.55563/clinexprheumatol/kr357t. Epub 2020 Sep 16. Clin Exp Rheumatol. 2021. PMID: 32940211
-
Pediatric-onset Takayasu's arteritis: clinical features and short-term outcome.Rheumatol Int. 2015 Oct;35(10):1701-6. doi: 10.1007/s00296-015-3272-7. Epub 2015 Apr 24. Rheumatol Int. 2015. PMID: 25903354
-
Assessment of damage in Takayasu's arteritis.Semin Arthritis Rheum. 2020 Aug;50(4):586-591. doi: 10.1016/j.semarthrit.2020.04.003. Epub 2020 May 14. Semin Arthritis Rheum. 2020. PMID: 32470706
-
Small vessel involvement in Takayasu's arteritis.Autoimmun Rev. 2013 Jan;12(3):355-62. doi: 10.1016/j.autrev.2012.05.010. Epub 2012 Jun 9. Autoimmun Rev. 2013. PMID: 22691438 Review.
-
Updates in the diagnosis and management of Takayasu's arteritis.Postgrad Med. 2023 Jan;135(sup1):14-21. doi: 10.1080/00325481.2022.2159723. Epub 2023 Jan 2. Postgrad Med. 2023. PMID: 36588528 Review.
Cited by
-
Cerebrovascular involvement in systemic childhood vasculitides.Clin Rheumatol. 2023 Oct;42(10):2733-2746. doi: 10.1007/s10067-023-06552-5. Epub 2023 Mar 8. Clin Rheumatol. 2023. PMID: 36884156 Review.
-
A Glimpse into Humoral Response and Related Therapeutic Approaches of Takayasu's Arteritis.Int J Mol Sci. 2024 Jun 13;25(12):6528. doi: 10.3390/ijms25126528. Int J Mol Sci. 2024. PMID: 38928233 Free PMC article. Review.
-
Advances in Takayasu arteritis: An Asia Pacific perspective.Front Med (Lausanne). 2022 Aug 15;9:952972. doi: 10.3389/fmed.2022.952972. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36045929 Free PMC article. Review.
-
Clinical characteristics and risk factors of coronary artery lesions in chinese pediatric Takayasu arteritis patients: a retrospective study.Pediatr Rheumatol Online J. 2023 Apr 28;21(1):42. doi: 10.1186/s12969-023-00820-z. Pediatr Rheumatol Online J. 2023. PMID: 37118779 Free PMC article.
-
Chinese guideline for the diagnosis and treatment of Takayasu's arteritis (2023).Rheumatol Immunol Res. 2024 Mar 31;5(1):5-26. doi: 10.1515/rir-2024-0002. eCollection 2024 Mar. Rheumatol Immunol Res. 2024. PMID: 38571931 Free PMC article. Review.
References
-
- Numano F, Kakatu T.. Takayasu arteritis—five doctors in the history of Takayasu arteritis. Int J Cardiol 1996;54:S1–10. - PubMed
-
- Numano F. The story of Takayasu arteritis. Rheumatology 2002;41:103–6. - PubMed
-
- Kerr GS, Hallahan CW, Giordano J. et al. Takayasu arteritis. Ann Intern Med 1994;120:919–29. - PubMed
-
- Valsakumar AK, Valappil UC, Jorapur V. et al. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol 2003;30:1793–8. - PubMed
-
- Yang L, Zhang H, Jiang X. et al. Clinical manifestations and longterm outcome for patients with Takayasu arteritis in China. J Rheumatol 2014;41:2439–46. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
