

Long-Term Respiratory and Neurological Sequelae of COVID-19
- PMID: 33177481
- PMCID: PMC7643287
- DOI: 10.12659/MSM.928996
Long-Term Respiratory and Neurological Sequelae of COVID-19
Abstract
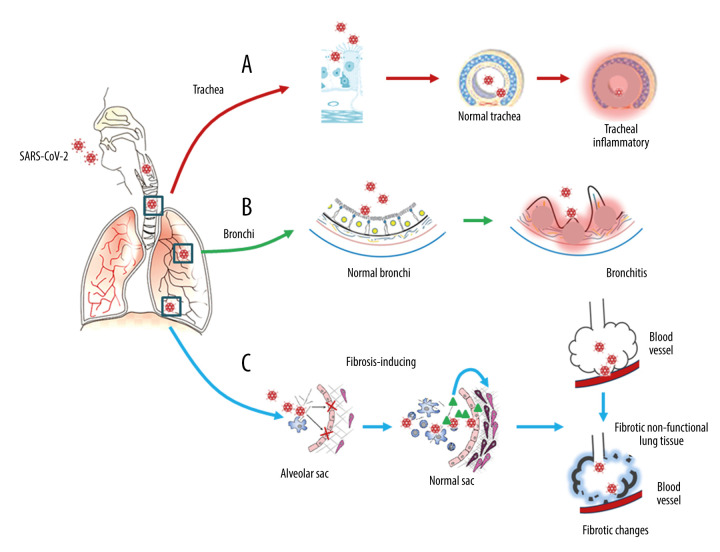
Since the initial reports of coronavirus disease 2019 (COVID-19) in China in late 2019, infections from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have spread rapidly, resulting in a global pandemic that has caused millions of deaths. Initially, the large number of infected people required the direction of global healthcare resources to provide supportive care for the acutely ill population in an attempt to reduce mortality. While clinical trials for safe and effective antiviral agents are ongoing, and vaccine development programs are being accelerated, long-term sequelae of SARS-CoV-2 infection have become increasingly recognized and concerning. Although the upper and lower respiratory tracts are the main sites of entry of SARS-CoV-2 into the body, resulting in COVID-19 pneumonia as the most common presentation, acute lung damage may be followed by pulmonary fibrosis and chronic impairment of lung function, with impaired quality of life. Also, increasing reports have shown that SARS-CoV-2 infection involves the central nervous system (CNS) and the peripheral nervous system (PNS) and directly or indirectly damages neurons, leading to long-term neurological sequelae. This review aims to provide an update on the mechanisms involved in the development of the long-term sequelae of SARS-CoV-2 infection in the 3 main areas of lung injury, neuronal injury, and neurodegenerative diseases, including Alzheimer disease, Parkinson disease, and multiple sclerosis, and highlights the need for patient monitoring following the acute stage of infection with SARS-CoV-2 to provide a rationale for the prevention, diagnosis, and management of these potential long-term sequelae.
Conflict of interest statement
None.
Figures

Similar articles
-
Biomedical Perspectives of Acute and Chronic Neurological and Neuropsychiatric Sequelae of COVID-19.Curr Neuropharmacol. 2022;20(6):1229-1240. doi: 10.2174/1570159X20666211223130228. Curr Neuropharmacol. 2022. PMID: 34951387 Free PMC article.
-
Emerging COVID-19 Neurological Manifestations: Present Outlook and Potential Neurological Challenges in COVID-19 Pandemic.Mol Neurobiol. 2021 Sep;58(9):4694-4715. doi: 10.1007/s12035-021-02450-6. Epub 2021 Jun 24. Mol Neurobiol. 2021. PMID: 34169443 Free PMC article. Review.
-
Long-term complications after infection with SARS-CoV-1, influenza and MERS-CoV - Lessons to learn in long COVID?Infect Dis Now. 2023 Oct;53(8):104779. doi: 10.1016/j.idnow.2023.104779. Epub 2023 Sep 9. Infect Dis Now. 2023. PMID: 37678512 Review.
-
Three Cases of COVID-19 Pneumonia in Female Patients in Italy Who Had Pulmonary Fibrosis on Follow-Up Lung Computed Tomography Imaging.Am J Case Rep. 2020 Nov 21;21:e926921. doi: 10.12659/AJCR.926921. Am J Case Rep. 2020. PMID: 33219200 Free PMC article.
-
Healing after COVID-19: are survivors at risk for pulmonary fibrosis?Am J Physiol Lung Cell Mol Physiol. 2021 Feb 1;320(2):L257-L265. doi: 10.1152/ajplung.00238.2020. Epub 2020 Dec 23. Am J Physiol Lung Cell Mol Physiol. 2021. PMID: 33355522 Free PMC article. Review.
Cited by
-
COVID-19: Unveiling the Neuropsychiatric Maze-From Acute to Long-Term Manifestations.Biomedicines. 2024 May 22;12(6):1147. doi: 10.3390/biomedicines12061147. Biomedicines. 2024. PMID: 38927354 Free PMC article. Review.
-
Muscle dysfunction in the long coronavirus disease 2019 syndrome: Pathogenesis and clinical approach.Rev Med Virol. 2022 Nov;32(6):e2355. doi: 10.1002/rmv.2355. Epub 2022 Apr 13. Rev Med Virol. 2022. PMID: 35416359 Free PMC article. Review.
-
Common Molecular Pathways Between Post-COVID19 Syndrome and Lung Fibrosis: A Scoping Review.Front Pharmacol. 2022 Mar 4;13:748931. doi: 10.3389/fphar.2022.748931. eCollection 2022. Front Pharmacol. 2022. PMID: 35308222 Free PMC article. Review.
-
Functional reprogramming of monocytes in patients with acute and convalescent severe COVID-19.JCI Insight. 2022 Apr 5;7(9):e154183. doi: 10.1172/jci.insight.154183. JCI Insight. 2022. PMID: 35380990 Free PMC article.
-
COVID-19-induced pulmonary sarcoid: A case report and review of the literature.Clin Imaging. 2022 Mar;83:152-158. doi: 10.1016/j.clinimag.2021.12.021. Epub 2022 Jan 13. Clin Imaging. 2022. PMID: 35051738 Free PMC article. Review.
References
-
- Kannan S, Shaik Syed Ali P, Sheeza A, Hemalatha K. COVID-19 (Novel Coronavirus 2019) – recent trends. Eur Rev Med Pharmacol Sci. 2020;24(4):2006–11. - PubMed
-
- Oldfield E, Malwal SR. COVID-19 and other pandemics: How might they be prevented? ACS Infect Dis. 2020;6(7):1563–66. - PubMed
-
- Helms J, Tacquard C, Severac F, et al. CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis) High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020;46(6):1089–98. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
