

Burden of non-communicable diseases from infectious causes in 2017: a modelling study
- PMID: 33098769
- PMCID: PMC8040338
- DOI: 10.1016/S2214-109X(20)30358-2
Burden of non-communicable diseases from infectious causes in 2017: a modelling study
Abstract
Background: Non-communicable diseases (NCDs) cause a large burden of disease globally. Some infectious diseases cause an increased risk of developing specific NCDs. Although the NCD burden from some infectious causes has been quantified, in this study, we aimed to more comprehensively quantify the global burden of NCDs from infectious causes.
Methods: In this modelling study, we identified NCDs with established infectious risk factors and infectious diseases with long-term non-communicable sequelae, and did narrative reviews between April 11, 2018, and June 10, 2020, to obtain relative risks (RRs) or population attributable fractions (PAFs) from studies quantifying the contribution of infectious causes to NCDs. To determine infection-attributable burden for the year 2017, we applied estimates of PAFs to estimates of disease burden from the Global Burden of Disease Study (GBD) 2017 for pairs of infectious causes and NCDs, or used estimates of attributable burden directly from GBD 2017. Morbidity and mortality burden from these conditions was summarised with age-standardised rates of disability-adjusted life-years (DALYs), for geographical regions as defined by the GBD. Estimates of NCD burden attributable to infectious causes were compared with attributable burden for the groups of risk factors with the highest PAFs from GBD 2017.
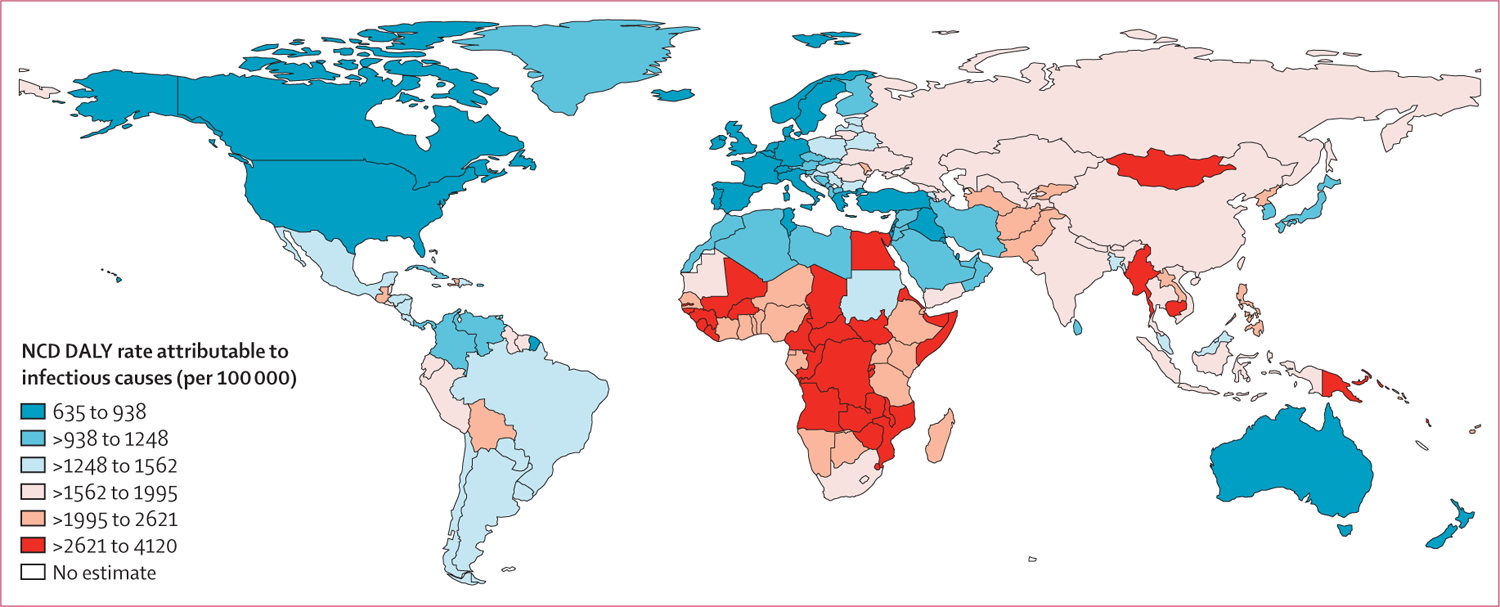
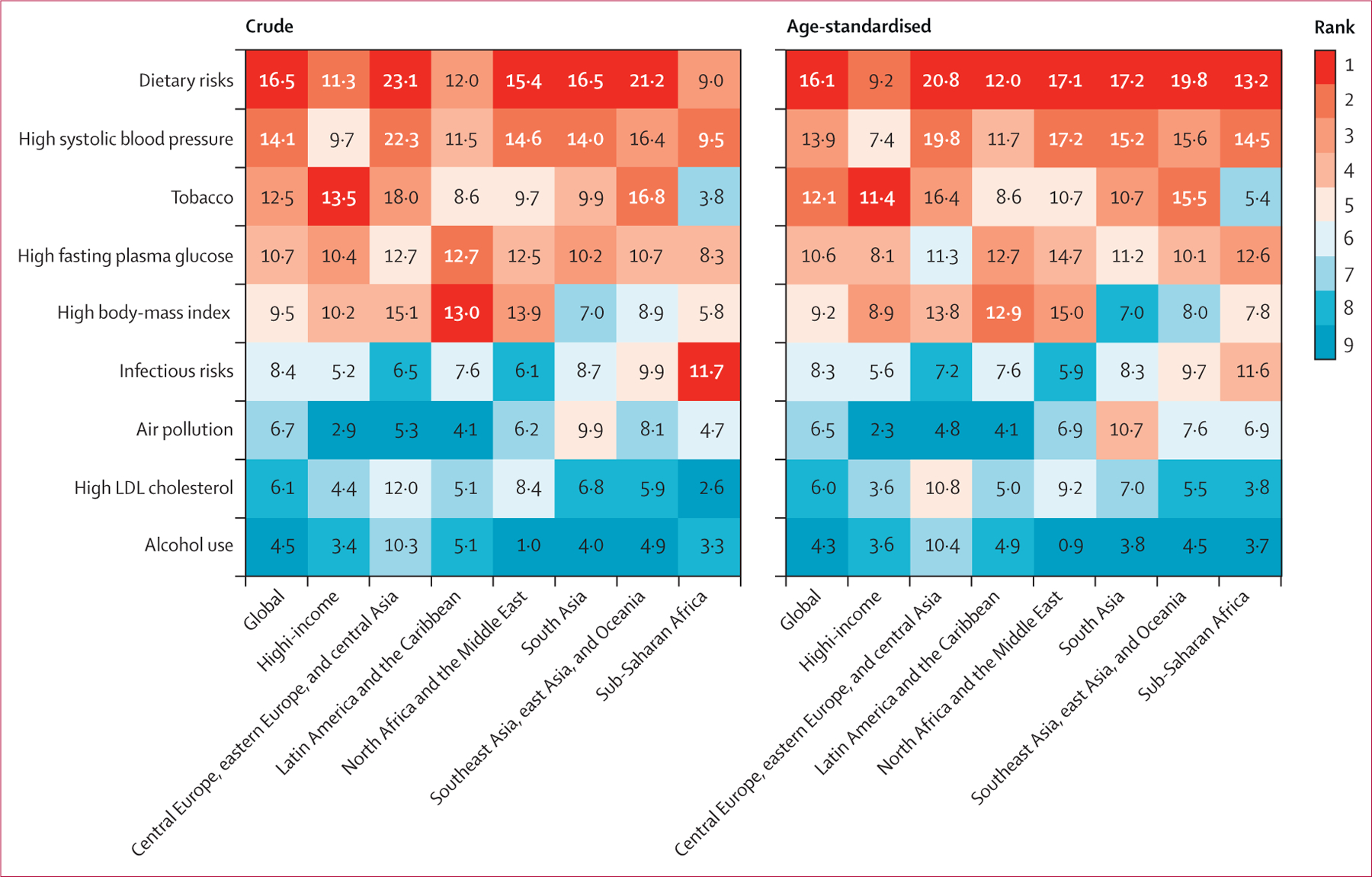
Findings: Globally, we quantified 130 million DALYs from NCDs attributable to infection, comprising 8·4% of all NCD DALYs. The infection-NCD pairs with the largest burden were gastric cancer due to H pylori (14·6 million DALYs), cirrhosis and other chronic liver diseases due to hepatitis B virus (12·2 million) and hepatitis C virus (10·4 million), liver cancer due to hepatitis B virus (9·4 million), rheumatic heart disease due to streptococcal infection (9·4 million), and cervical cancer due to HPV (8·0 million). Age-standardised rates of infection-attributable NCD burden were highest in Oceania (3564 DALYs per 100 000 of the population) and central sub-Saharan Africa (2988 DALYs per 100 000) followed by the other sub-Saharan African regions, and lowest in Australia and New Zealand (803 DALYs per 100 000) followed by other high-income regions. In sub-Saharan Africa, the proportion of crude NCD burden attributable to infectious causes was 11·7%, which was higher than the proportion of burden attributable to each of several common risk factors of NCDs (tobacco, alcohol use, high systolic blood pressure, dietary risks, high fasting plasma glucose, air pollution, and high LDL cholesterol). In other broad regions, infectious causes ranked between fifth and eighth in terms of crude attributable proportions among the nine risks compared. The age-standardised attributable proportion for infectious risks remained highest in sub-Saharan Africa of the broad regions, but age-standardisation caused infectious risks to fall below dietary risks, high systolic blood pressure, and fasting plasma glucose in ranked attributable proportions within the region.
Interpretation: Infectious conditions cause substantial NCD burden with clear regional variation, and estimates of this burden are likely to increase as evidence that can be used for quantification expands. To comprehensively avert NCD burden, particularly in low-income and middle-income countries, the availability, coverage, and quality of cost-effective interventions for key infectious conditions need to be strengthened. Efforts to promote universal health coverage must address infectious risks leading to NCDs, particularly in populations with high rates of these infectious conditions, to reduce existing regional disparities in rates of NCD burden.
Funding: Leona M and Harry B Helmsley Charitable Trust.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
All other authors declare no competing interests.
Figures

Similar articles
-
Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results from the Global Burden of Disease Study 2017.Lancet Glob Health. 2019 Oct;7(10):e1375-e1387. doi: 10.1016/S2214-109X(19)30374-2. Lancet Glob Health. 2019. PMID: 31537368
-
Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017.Lancet. 2018 Nov 10;392(10159):1923-1994. doi: 10.1016/S0140-6736(18)32225-6. Epub 2018 Nov 8. Lancet. 2018. PMID: 30496105 Free PMC article.
-
Burden and trend of diet-related non-communicable diseases in Australia and comparison with 34 OECD countries, 1990-2015: findings from the Global Burden of Disease Study 2015.Eur J Nutr. 2019 Apr;58(3):1299-1313. doi: 10.1007/s00394-018-1656-7. Epub 2018 Mar 7. Eur J Nutr. 2019. PMID: 29516222
-
Excess Mortality from Mental, Neurological, and Substance Use Disorders in the Global Burden of Disease Study 2010.In: Patel V, Chisholm D, Dua T, Laxminarayan R, Medina-Mora ME, editors. Mental, Neurological, and Substance Use Disorders: Disease Control Priorities, Third Edition (Volume 4). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Mar 14. Chapter 3. In: Patel V, Chisholm D, Dua T, Laxminarayan R, Medina-Mora ME, editors. Mental, Neurological, and Substance Use Disorders: Disease Control Priorities, Third Edition (Volume 4). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Mar 14. Chapter 3. PMID: 27227239 Free Books & Documents. Review.
-
Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010.Lancet. 2014 Jan 18;383(9913):245-54. doi: 10.1016/s0140-6736(13)61953-4. Lancet. 2014. PMID: 24449944 Free PMC article. Review.
Cited by
-
Population-Level Distribution, Risk Factors, and Burden of Mortality and Disability-Adjusted Life Years Attributable to Major Noncommunicable Diseases in Western Europe (1990-2021): Ecological Analysis.JMIR Public Health Surveill. 2024 Oct 17;10:e57840. doi: 10.2196/57840. JMIR Public Health Surveill. 2024. PMID: 39418779 Free PMC article.
-
Burden of metabolic syndrome in the global adult HIV-infected population: a systematic review and meta-analysis.BMC Public Health. 2024 Sep 28;24(1):2657. doi: 10.1186/s12889-024-20118-3. BMC Public Health. 2024. PMID: 39342258 Free PMC article.
-
Presence of Intestinal Parasites in Patients with Chronic Non-Communicable Diseases in Masaya (Nicaragua).Trop Med Infect Dis. 2024 Jul 30;9(8):171. doi: 10.3390/tropicalmed9080171. Trop Med Infect Dis. 2024. PMID: 39195609 Free PMC article.
-
What public health challenges and unmet medical needs would benefit from interdisciplinary collaboration in the EU? A survey and multi-stakeholder debate.Front Public Health. 2024 Jul 22;12:1417684. doi: 10.3389/fpubh.2024.1417684. eCollection 2024. Front Public Health. 2024. PMID: 39104886 Free PMC article.
-
C-reactive protein and high-sensitivity C-reactive protein levels in asymptomatic intestinal parasite carriers from urban and rural areas of Gabon.PLoS Negl Trop Dis. 2024 May 20;18(5):e0011282. doi: 10.1371/journal.pntd.0011282. eCollection 2024 May. PLoS Negl Trop Dis. 2024. PMID: 38768226 Free PMC article.
References
-
- WHO. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Geneva: World Health Organization, 2013. http://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.... (accessed Jan 15, 2020).
-
- UN General Assembly. Political declaration of the third high-level meeting of the General Assembly on the prevention and control of non-communicable diseases. A/RES/73/2. October 17, 2018. https://digitallibrary.un.org/record/1648984?ln=en (accessed Jan 15, 2020).
-
- Ravelli GP, Stein ZA, Susser MW. Obesity in young men after famine exposure in utero and early infancy. N Engl J Med 1976; 295: 349–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
