

Experimental murine arteriovenous fistula model to study restenosis after transluminal angioplasty
- PMID: 33082594
- PMCID: PMC8077734
- DOI: 10.1038/s41684-020-00659-x
Experimental murine arteriovenous fistula model to study restenosis after transluminal angioplasty
Abstract
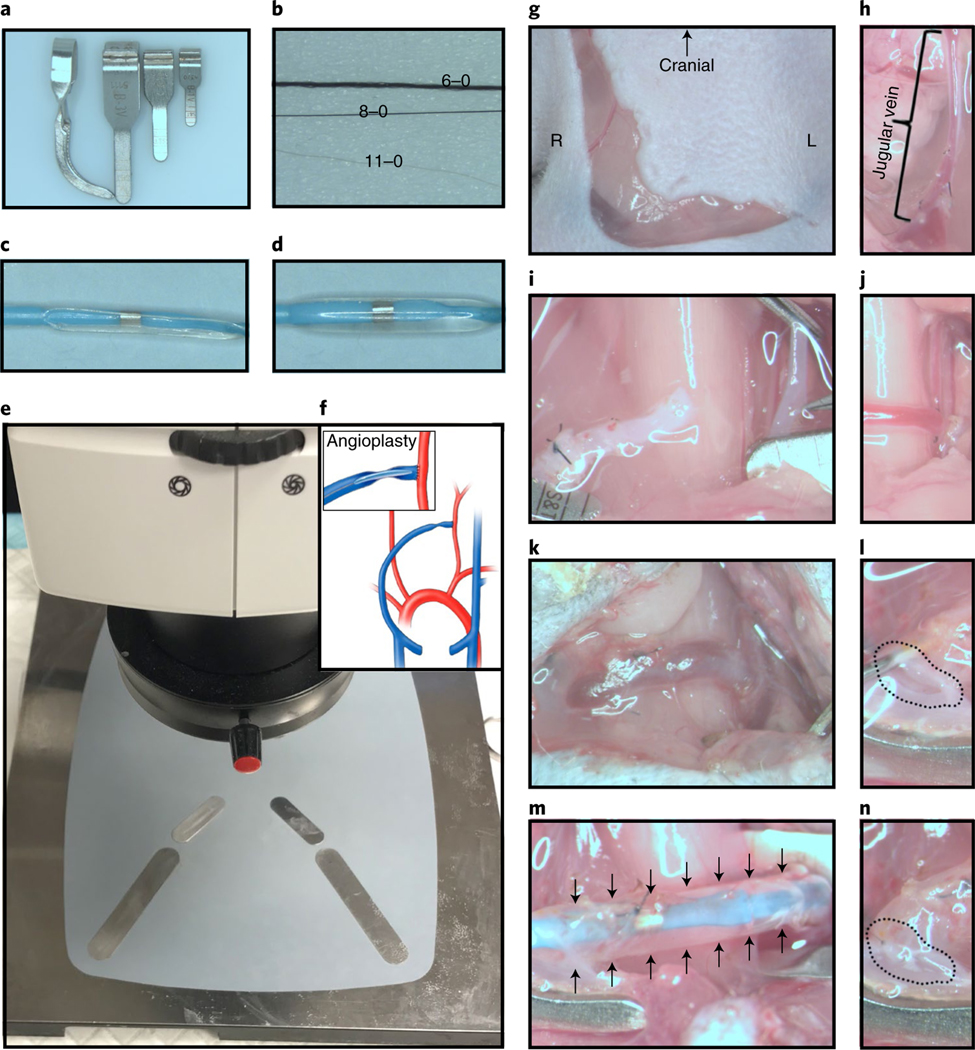
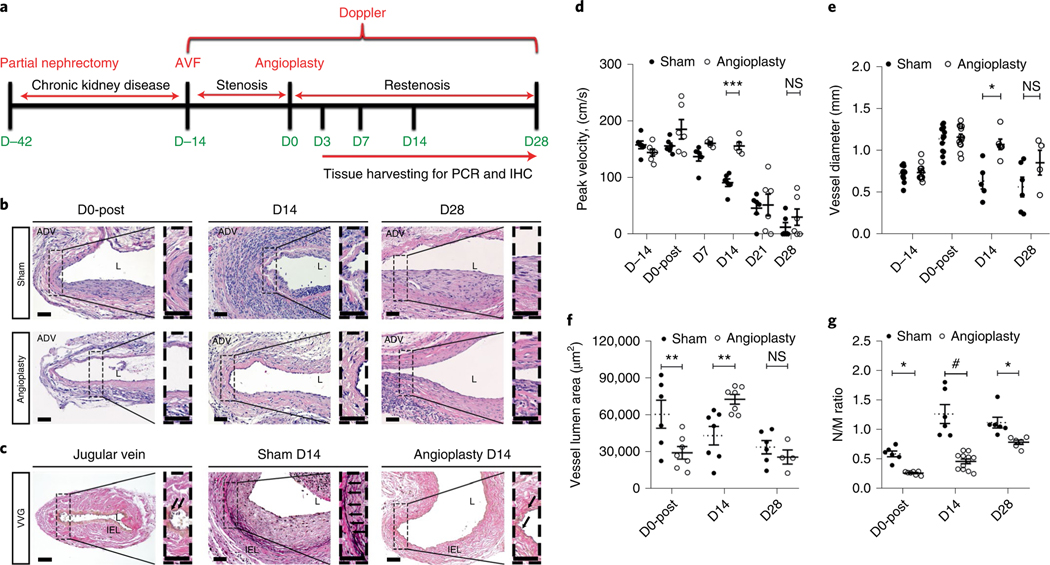
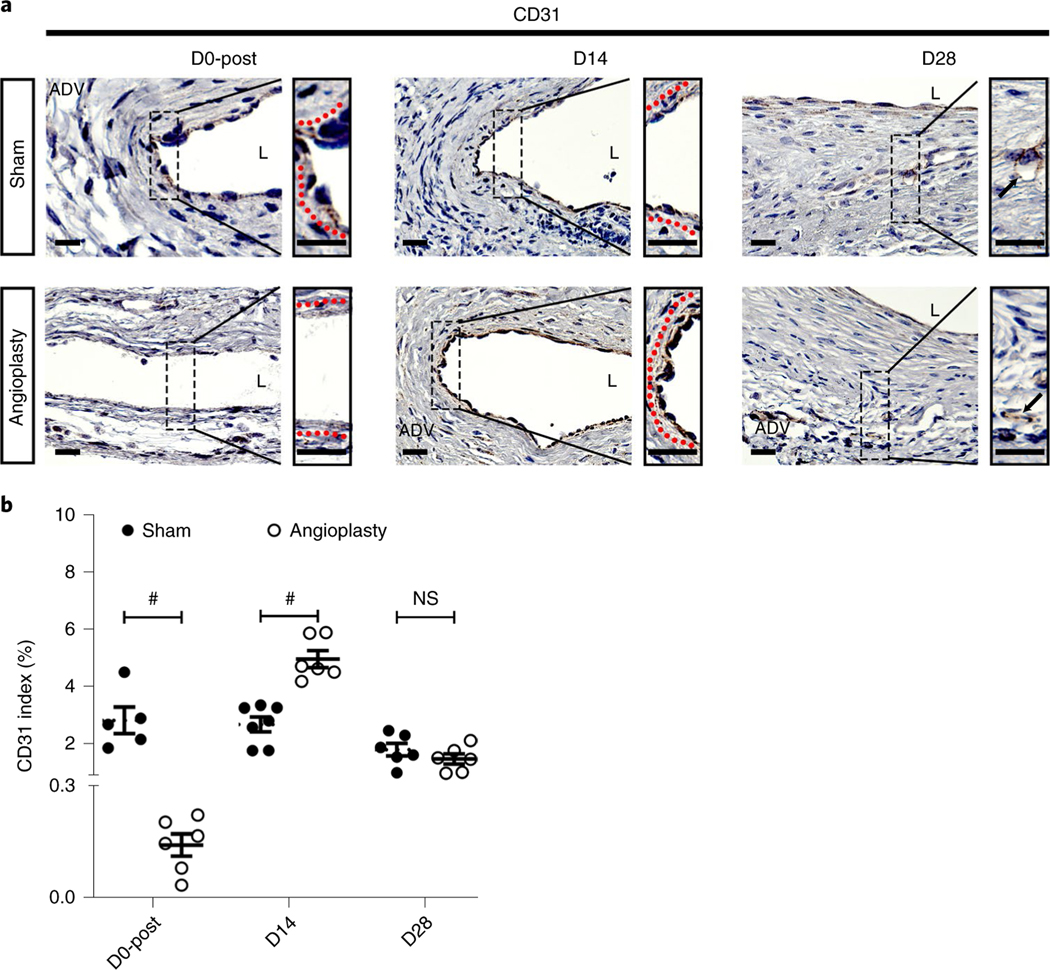
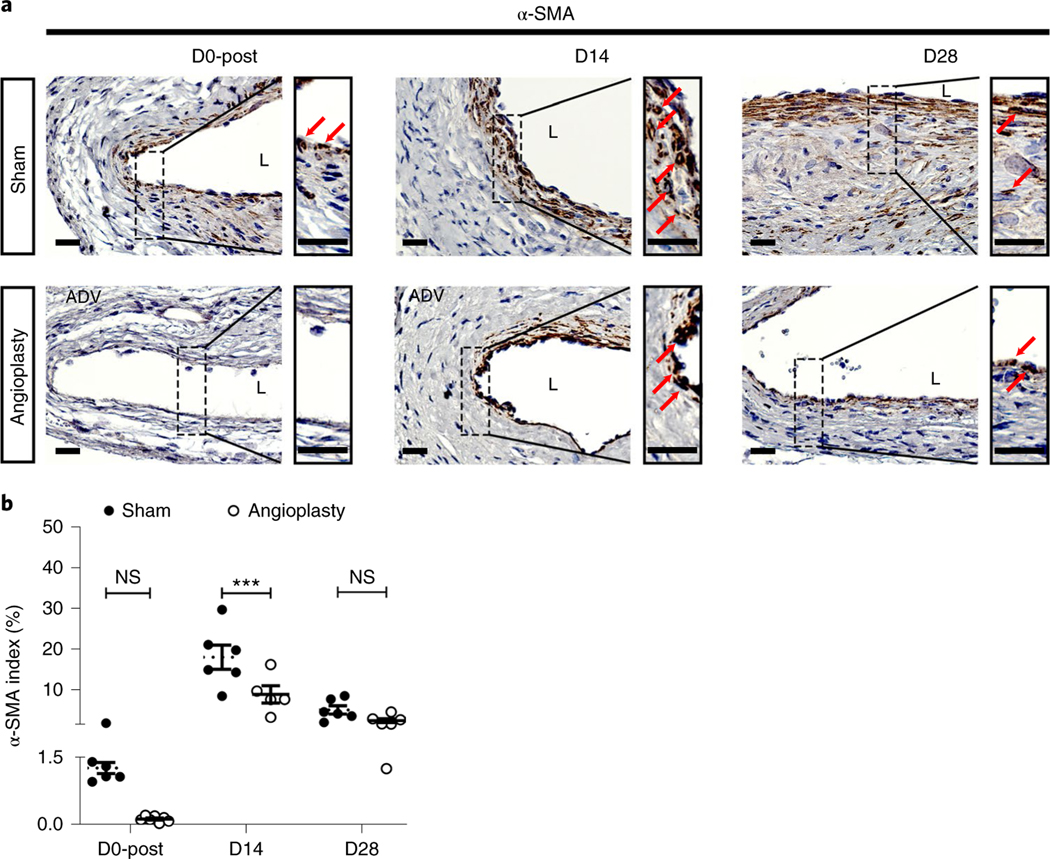
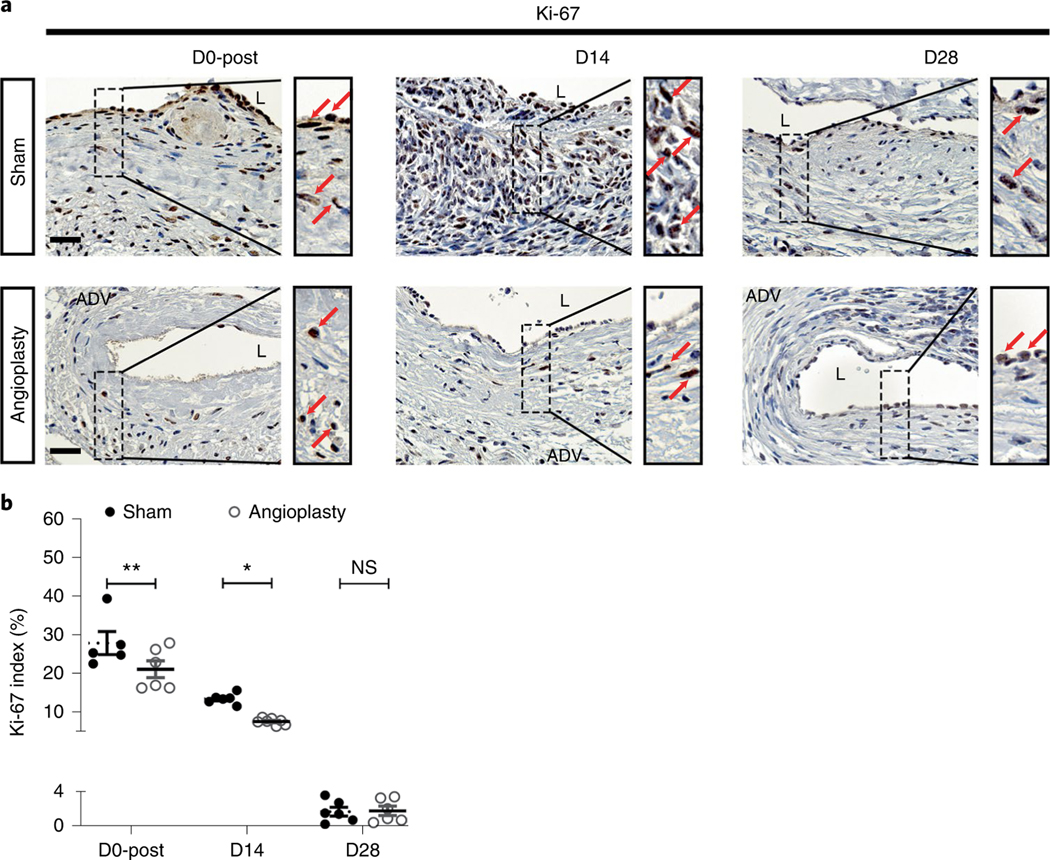
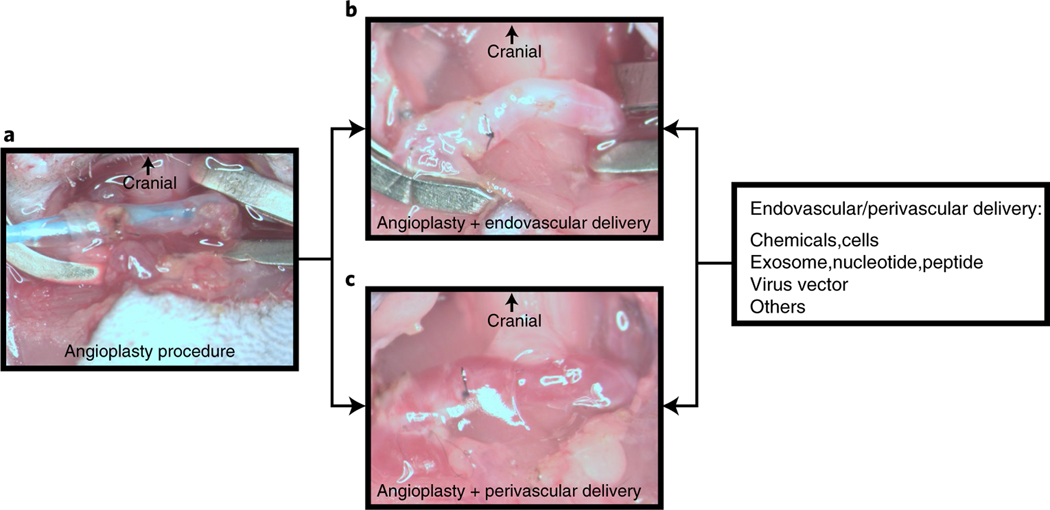
Percutaneous transluminal angioplasty (PTA) is a very common interventional treatment for treating stenosis in arteriovenous fistula (AVF) used for hemodialysis vascular access. Restenosis occurs after PTA, resulting in vascular lumen loss and a decrease in blood flow. Experimental animal models have been developed to study the pathogenesis of stenosis, but there is no restenosis model after PTA of stenotic AVF in mice. Here, we describe the creation of a murine model of restenosis after angioplasty of a stenosis in an AVF. The murine restenosis model has several advantages, including the rapid development of restenotic lesions in the vessel after angioplasty and the potential to evaluate endovascular and perivascular therapeutics for treating restenosis. The protocol includes a detailed description of the partial nephrectomy procedure to induce chronic kidney disease, the AVF procedure for development of de novo stenosis and the angioplasty treatment associated with progression of restenosis. We monitored the angioplasty-treated vessel for vascular patency and hemodynamic changes for a period of 28 d using ultrasound. Vessels were collected at different time points and processed for histological analysis and immunostaining. This angioplasty model, which can be performed with basic microvascular surgery skills, could be used to identify potential endovascular and perivascular therapies to reduce restenosis after angioplasty procedures.
Figures
Similar articles
-
The efficacy of percutaneous transluminal angioplasty and arteriovenous fistula reconstruction for immature arteriovenous fistula.BMC Nephrol. 2023 Oct 17;24(1):304. doi: 10.1186/s12882-023-03361-5. BMC Nephrol. 2023. PMID: 37848833 Free PMC article.
-
Calcium channel antagonists reduce restenosis after percutaneous transluminal angioplasty of an arteriovenous fistula in hemodialysis patients.Ther Apher Dial. 2008 Jun;12(3):232-6. doi: 10.1111/j.1744-9987.2008.00579.x. Ther Apher Dial. 2008. PMID: 18503701
-
Ultrasound-guided percutaneous endovascular treatment of arteriovenous fistula/graft.Clin Nephrol. 2017 Supplement 1;88(13):61-64. doi: 10.5414/CNP88FX15. Clin Nephrol. 2017. PMID: 28655388
-
[Triple stenosis of brachio-basilic arteriovenous fistula: percutaneous transluminal angioplasty utility, case report and literature review].G Ital Nefrol. 2022 Oct 31;39(5):2022-vol5. G Ital Nefrol. 2022. PMID: 36563076 Review. Italian.
-
[The new frontier in endovascular treatment of arteriovenous fistula stenosis: the role of ultrasound-guided percutaneous transluminal angioplasty].G Ital Nefrol. 2019 Apr;36(2):2019-vol2. G Ital Nefrol. 2019. PMID: 30983175 Review. Italian.
Cited by
-
The rodent models of arteriovenous fistula.Front Cardiovasc Med. 2024 Jan 18;11:1293568. doi: 10.3389/fcvm.2024.1293568. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38304139 Free PMC article. Review.
-
Posttraumatic arteriovenous fistula of the lower extremity and the pathological characteristic-case series and literature review.J Surg Case Rep. 2023 Dec 7;2023(12):rjad636. doi: 10.1093/jscr/rjad636. eCollection 2023 Dec. J Surg Case Rep. 2023. PMID: 38076318 Free PMC article.
-
Intimal CD31-Positive Relative Surfaces Are Associated with Systemic Inflammatory Markers and Maturation of Arteriovenous Fistula in Dialysis Patients.J Clin Med. 2023 Jun 30;12(13):4419. doi: 10.3390/jcm12134419. J Clin Med. 2023. PMID: 37445452 Free PMC article.
-
The efficacy of percutaneous transluminal angioplasty and arteriovenous fistula reconstruction for immature arteriovenous fistula.BMC Nephrol. 2023 Oct 17;24(1):304. doi: 10.1186/s12882-023-03361-5. BMC Nephrol. 2023. PMID: 37848833 Free PMC article.
-
Animal Models of Neointimal Hyperplasia and Restenosis: Species-Specific Differences and Implications for Translational Research.JACC Basic Transl Sci. 2021 Aug 11;6(11):900-917. doi: 10.1016/j.jacbts.2021.06.006. eCollection 2021 Nov. JACC Basic Transl Sci. 2021. PMID: 34869956 Free PMC article. Review.
References
-
- Al-Jaishi AA et al. Patency rates of the arteriovenous fistula for hemodialysis: a systematic review and meta-analysis. Am. J. Kidney Dis 63, 464–478 (2014). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
