

How We Treat Fever and Hypotension in Pediatric Hematopoietic Cell Transplant Patients
- PMID: 33042850
- PMCID: PMC7526343
- DOI: 10.3389/fonc.2020.581447
How We Treat Fever and Hypotension in Pediatric Hematopoietic Cell Transplant Patients
Abstract
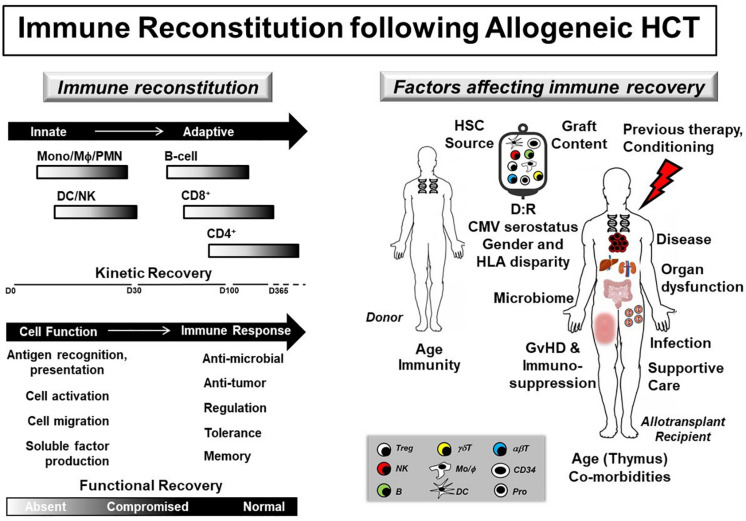
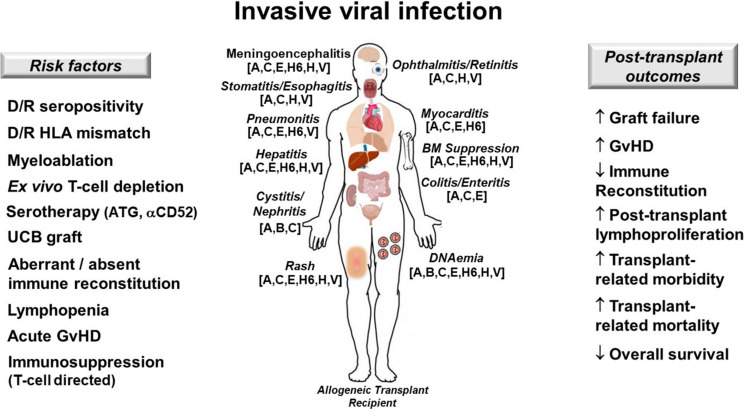
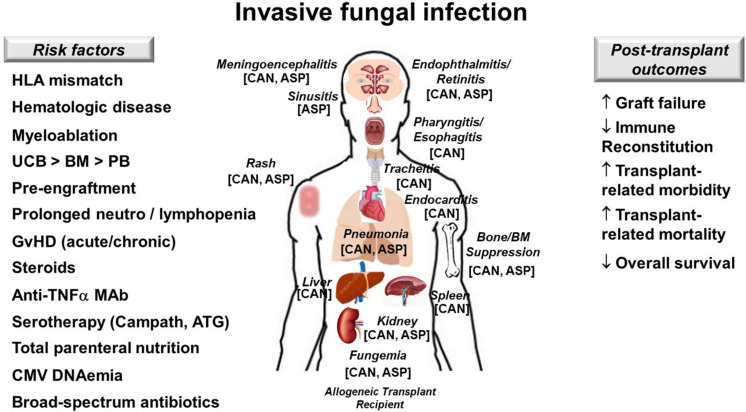
Pediatric allogeneic hematopoietic cell transplant (HCT) survival is limited by the development of post-transplant infections. In this overview, we discuss a clinical approach to the prompt recognition and treatment of fever and hypotension in pediatric HCT patients. Special attention is paid to individualized hemodynamic resuscitation, thorough diagnostic testing, novel anti-pathogen therapies, and the multimodal support required for recovery. We present three case vignettes that illustrate the complexities of post-HCT sepsis and highlight best practices that contribute to optimal transplant survival in children.
Keywords: bone marrow transplant; fever; hypotension; infection; sepsis.
Copyright © 2020 Zinter, Dvorak and Auletta.
Figures

Similar articles
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
Allogeneic hematopoietic cell transplantation (allogeneic HCT) for treatment of pediatric Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL).Pediatr Blood Cancer. 2009 Dec 15;53(7):1289-94. doi: 10.1002/pbc.22263. Pediatr Blood Cancer. 2009. PMID: 19731318
-
Risk Factors for Subsequent Central Nervous System Tumors in Pediatric Allogeneic Hematopoietic Cell Transplant: A Study from the Center for International Blood and Marrow Transplant Research (CIBMTR).Biol Blood Marrow Transplant. 2017 Aug;23(8):1320-1326. doi: 10.1016/j.bbmt.2017.04.004. Epub 2017 Apr 12. Biol Blood Marrow Transplant. 2017. PMID: 28411175 Free PMC article. Clinical Trial.
-
Venous Thromboembolism in Pediatric Hematopoietic Cell Transplant: A Multicenter Cohort Study.Biol Blood Marrow Transplant. 2018 Feb;24(2):337-342. doi: 10.1016/j.bbmt.2017.10.038. Epub 2017 Nov 8. Biol Blood Marrow Transplant. 2018. PMID: 29128552
-
Transplant-Associated Thrombotic Microangiopathy in Pediatric Hematopoietic Cell Transplant Recipients: A Practical Approach to Diagnosis and Management.Front Pediatr. 2019 Apr 9;7:133. doi: 10.3389/fped.2019.00133. eCollection 2019. Front Pediatr. 2019. PMID: 31024873 Free PMC article. Review.
Cited by
-
Analysis of incidence and risk factors of the multidrug resistant gastrointestinal tract infection in children and adolescents undergoing allogeneic and autologous hematopoietic cell transplantation: a nationwide study.Ann Hematol. 2022 Jan;101(1):191-201. doi: 10.1007/s00277-021-04681-y. Epub 2021 Oct 21. Ann Hematol. 2022. PMID: 34674000 Free PMC article.
References
-
- Lindell RB, Gertz SJ, Rowan CM, McArthur J, Beske F, Plunkett A, et al. High levels of morbidity and mortality among pediatric hematopoietic cell transplant recipients with severe sepsis: insights from the sepsis PRevalence, OUtcomes, and therapies International point prevalence study. Pediatr Crit Care Med. (2017) 18:1114–25. 10.1097/PCC.0000000000001338 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources