

Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque
- PMID: 33003973
- PMCID: PMC7736526
- DOI: 10.1161/CIRCULATIONAHA.120.049981
Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque
Abstract
Background: Immune checkpoint inhibitors (ICIs) treat an expanding range of cancers. Consistent basic data suggest that these same checkpoints are critical negative regulators of atherosclerosis. Therefore, our objectives were to test whether ICIs were associated with accelerated atherosclerosis and a higher risk of atherosclerosis-related cardiovascular events.
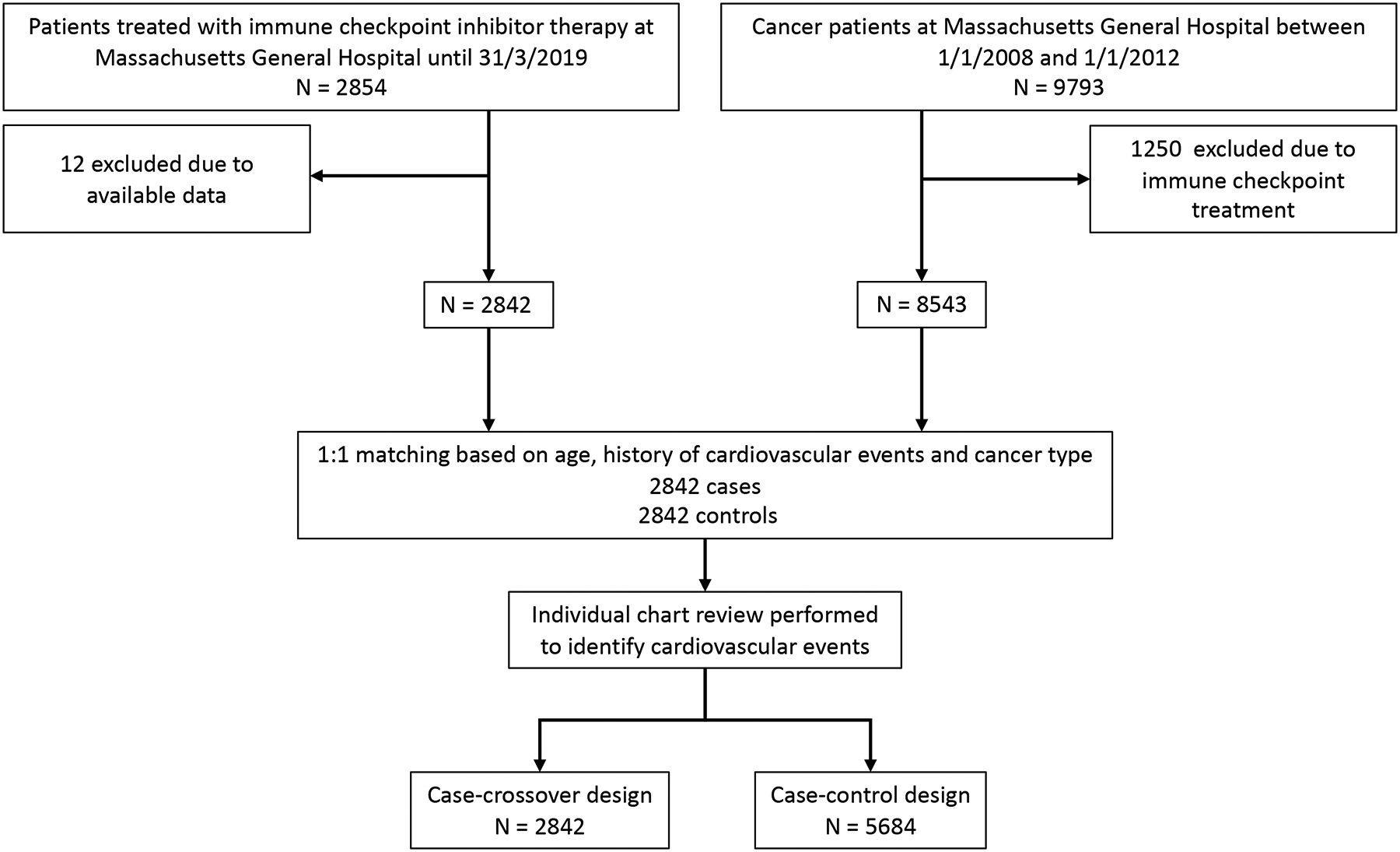
Methods: The study was situated in a single academic medical center. The primary analysis evaluated whether exposure to an ICI was associated with atherosclerotic cardiovascular events in 2842 patients and 2842 controls matched by age, a history of cardiovascular events, and cancer type. In a second design, a case-crossover analysis was performed with an at-risk period defined as the 2-year period after and the control period as the 2-year period before treatment. The primary outcome was a composite of atherosclerotic cardiovascular events (myocardial infarction, coronary revascularization, and ischemic stroke). Secondary outcomes included the individual components of the primary outcome. In addition, in an imaging substudy (n=40), the rate of atherosclerotic plaque progression was compared from before to after the ICI was started. All study measures and outcomes were blindly adjudicated.
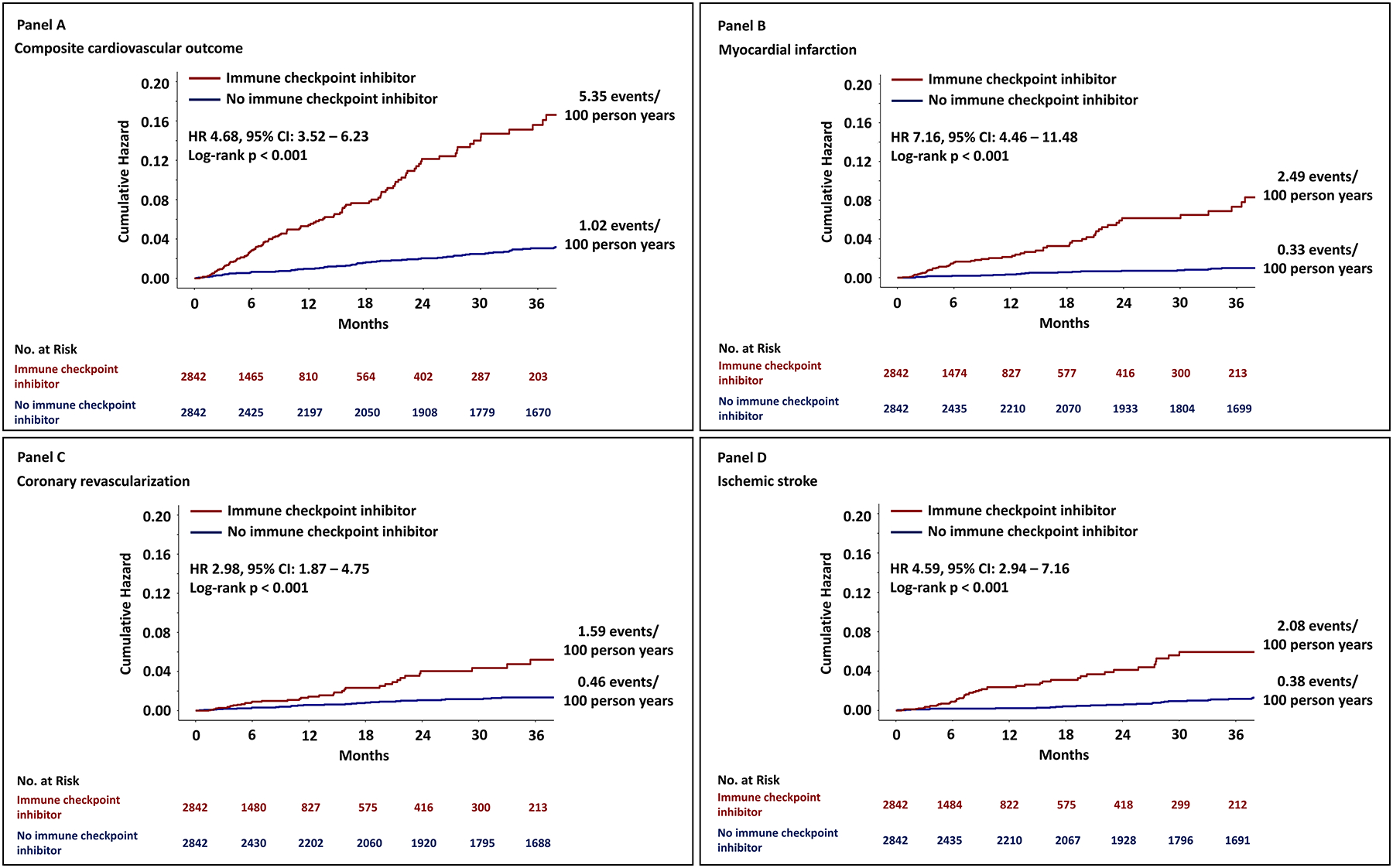
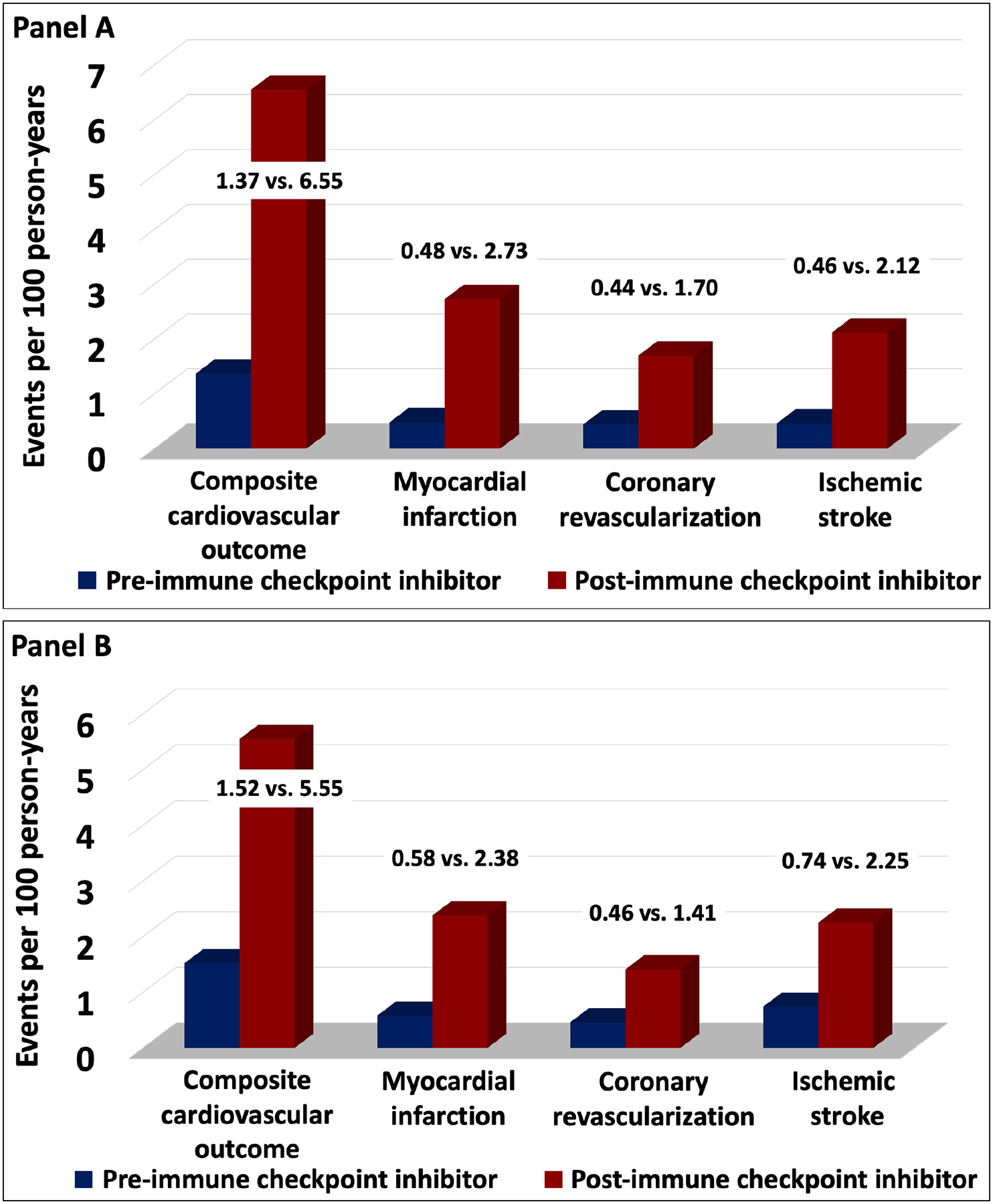
Results: In the matched cohort study, there was a 3-fold higher risk for cardiovascular events after starting an ICI (hazard ratio, 3.3 [95% CI, 2.0-5.5]; P<0.001). There was a similar increase in each of the individual components of the primary outcome. In the case-crossover, there was also an increase in cardiovascular events from 1.37 to 6.55 per 100 person-years at 2 years (adjusted hazard ratio, 4.8 [95% CI, 3.5-6.5]; P<0.001). In the imaging study, the rate of progression of total aortic plaque volume was >3-fold higher with ICIs (from 2.1%/y before 6.7%/y after). This association between ICI use and increased atherosclerotic plaque progression was attenuated with concomitant use of statins or corticosteroids.
Conclusions: Cardiovascular events were higher after initiation of ICIs, potentially mediated by accelerated progression of atherosclerosis. Optimization of cardiovascular risk factors and increased awareness of cardiovascular risk before, during, and after treatment should be considered among patients on an ICI.
Keywords: atherosclerosis; immunomodulation; plaque, atherosclerotic.
Conflict of interest statement
Figures
Comment in
-
By Releasing the Brakes With Immunotherapy, Are We Accelerating Atherosclerosis?Circulation. 2020 Dec 15;142(24):2312-2315. doi: 10.1161/CIRCULATIONAHA.120.051753. Epub 2020 Dec 14. Circulation. 2020. PMID: 33315491 No abstract available.
-
Letter by Sarayani et al Regarding Article, "Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque".Circulation. 2021 Jun 22;143(25):e1031-e1032. doi: 10.1161/CIRCULATIONAHA.120.052678. Epub 2021 Jun 21. Circulation. 2021. PMID: 34152796 No abstract available.
-
Response to Sarayani et al Regarding Article, "Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque".Circulation. 2021 Jun 22;143(25):e1033-e1034. doi: 10.1161/CIRCULATIONAHA.121.054169. Epub 2021 Jun 21. Circulation. 2021. PMID: 34152798 Free PMC article. No abstract available.
Similar articles
-
Immune checkpoint inhibitors in cancer: the increased risk of atherosclerotic cardiovascular disease events and progression of coronary artery calcium.BMC Med. 2024 Jan 31;22(1):44. doi: 10.1186/s12916-024-03261-x. BMC Med. 2024. PMID: 38291431 Free PMC article.
-
Atherosclerotic Cardiovascular Events in Cancer Patients Treated With Immune Checkpoint Inhibitors: A Retrospective Cohort Study.Heart Lung Circ. 2024 May;33(5):721-729. doi: 10.1016/j.hlc.2023.10.008. Epub 2023 Dec 1. Heart Lung Circ. 2024. PMID: 38042638
-
Impact of immune checkpoint inhibitors on atherosclerosis progression in patients with lung cancer.J Immunother Cancer. 2023 Jul;11(7):e007307. doi: 10.1136/jitc-2023-007307. J Immunother Cancer. 2023. PMID: 37433718 Free PMC article.
-
An Increased Understanding of the Association Between Atherosclerosis and Immune Checkpoint Inhibitors.Curr Cardiol Rep. 2023 Aug;25(8):879-887. doi: 10.1007/s11886-023-01908-4. Epub 2023 Jul 3. Curr Cardiol Rep. 2023. PMID: 37395892 Review.
-
Immune checkpoint inhibitor treatment and atherosclerotic cardiovascular disease: an emerging clinical problem.J Immunother Cancer. 2021 Jun;9(6):e002916. doi: 10.1136/jitc-2021-002916. J Immunother Cancer. 2021. PMID: 34168005 Free PMC article. Review.
Cited by
-
Newly diagnosed cardiovascular disease in patients treated with immune checkpoint inhibitors: a retrospective analysis of patients at an academic tertiary care center.Cardiooncology. 2021 Mar 18;7(1):10. doi: 10.1186/s40959-021-00097-9. Cardiooncology. 2021. PMID: 33736707 Free PMC article.
-
Immune checkpoint inhibitors and the risk of major atherosclerotic cardiovascular events in patients with high-risk or advanced melanoma: a retrospective cohort study.Cardiooncology. 2022 Dec 2;8(1):23. doi: 10.1186/s40959-022-00149-8. Cardiooncology. 2022. PMID: 36461057 Free PMC article.
-
Immune Checkpoint Inhibitors Related to Cardiotoxicity.J Cardiovasc Dev Dis. 2022 Nov 3;9(11):378. doi: 10.3390/jcdd9110378. J Cardiovasc Dev Dis. 2022. PMID: 36354777 Free PMC article. Review.
-
Advances in immune checkpoint inhibitors induced-cardiotoxicity.Front Immunol. 2023 Feb 23;14:1130438. doi: 10.3389/fimmu.2023.1130438. eCollection 2023. Front Immunol. 2023. PMID: 36911712 Free PMC article. Review.
-
Effect of Aspirin on Melanoma Incidence in Older Persons: Extended Follow-up of a Large Randomized Double-blind Placebo-controlled Trial.Cancer Prev Res (Phila). 2022 Jun 2;15(6):365-375. doi: 10.1158/1940-6207.CAPR-21-0244. Cancer Prev Res (Phila). 2022. PMID: 35395069 Free PMC article. Clinical Trial.
References
-
- Tang J, Shalabi A and Hubbard-Lucey VM. Comprehensive analysis of the clinical immuno-oncology landscape. Ann Oncol. 2018;29:84–91. - PubMed
-
- Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, Haydon A, Lichinitser M, Khattak A, Carlino MS et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N Engl J Med. 2018;378:1789–1801. - PubMed
-
- Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2017;377:1919–1929. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
