

Immune dysfunction following COVID-19, especially in severe patients
- PMID: 32985562
- PMCID: PMC7522270
- DOI: 10.1038/s41598-020-72718-9
Immune dysfunction following COVID-19, especially in severe patients
Abstract
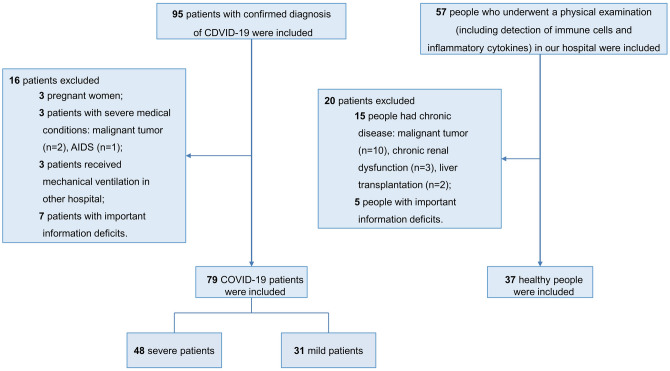
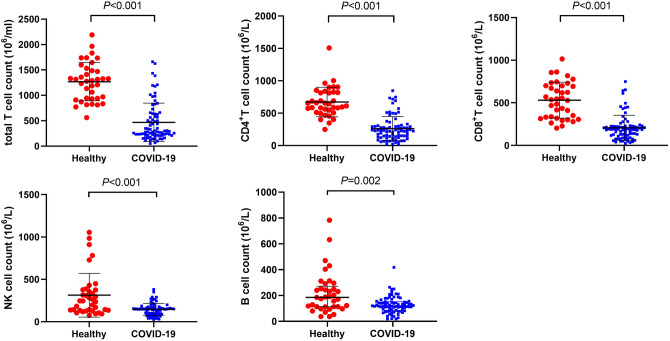
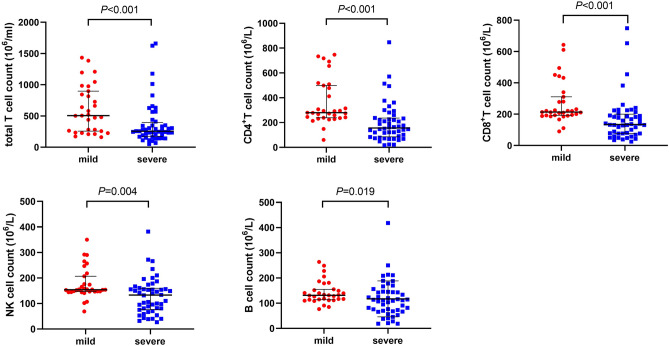
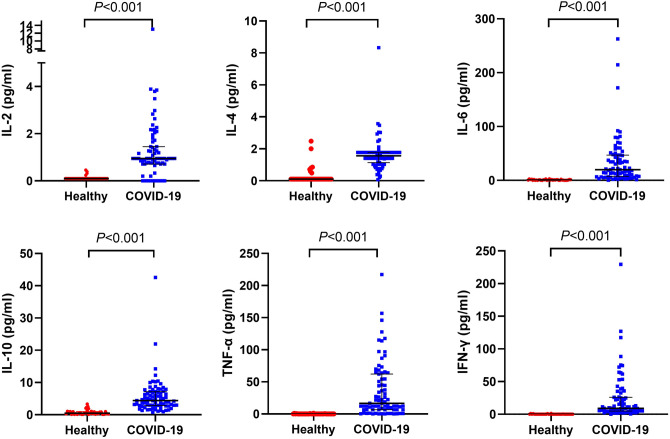
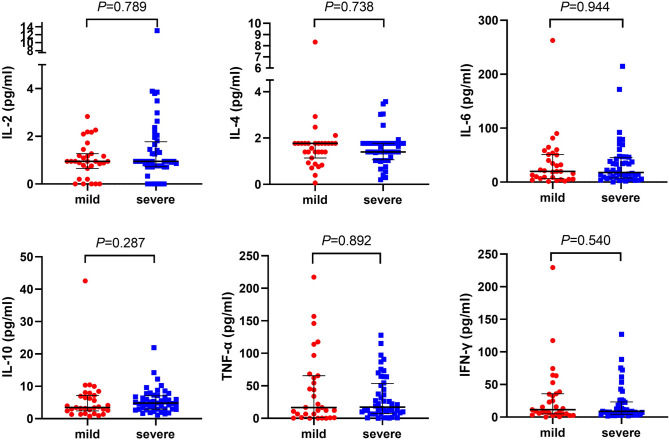
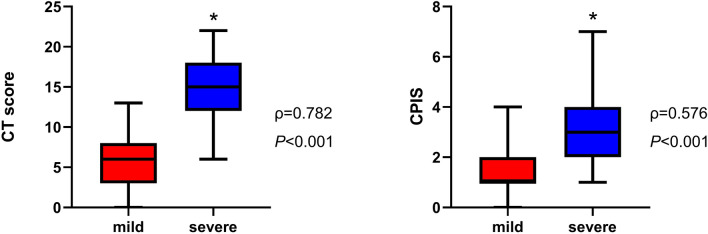
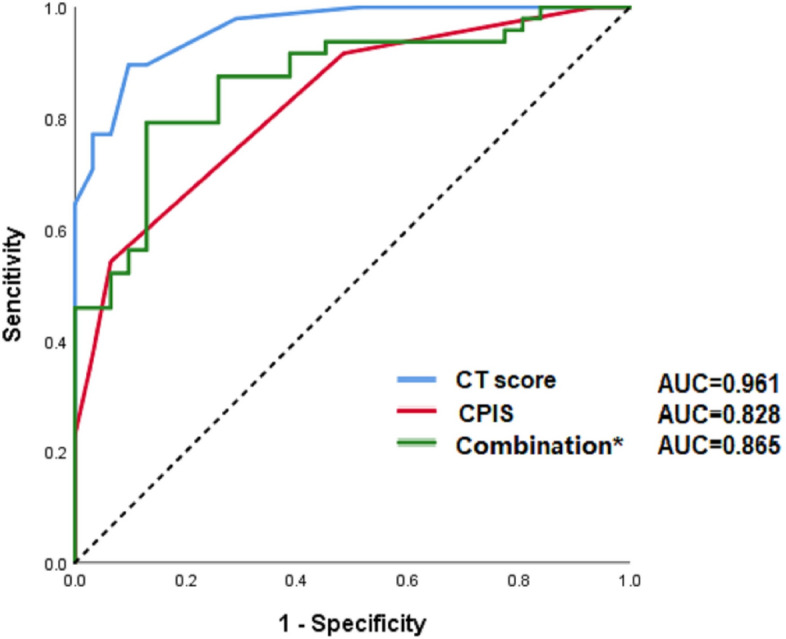
The coronavirus disease 2019 (COVID-19) has been spreading worldwide. Severe cases quickly progressed with unfavorable outcomes. We aim to investigate the clinical features of COVID-19 and identify the risk factors associated with its progression. Data of confirmed SARS-CoV-2-infected patients and healthy participants were collected. Thirty-seven healthy people and 79 confirmed patients, which include 48 severe patients and 31 mild patients, were recruited. COVID-19 patients presented with dysregulated immune response (decreased T, B, and NK cells and increased inflammatory cytokines). Also, they were found to have increased levels of white blood cell, neutrophil count, and D-dimer in severe cases. Moreover, lymphocyte, CD4+ T cell, CD8+ T cell, NK cell, and B cell counts were lower in the severe group. Multivariate logistic regression analysis showed that CD4+ cell count, neutrophil-to-lymphocyte ratio (NLR) and D-dimer were risk factors for severe cases. Both CT score and clinical pulmonary infection score (CPIS) were associated with disease severity. The receiver operating characteristic (ROC) curve analysis has shown that all these parameters and scores had quite a high predictive value. Immune dysfunction plays critical roles in disease progression. Early and constant surveillance of complete blood cell count, T lymphocyte subsets, coagulation function, CT scan and CPIS was recommended for early screening of severe cases.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical Characteristics and Immune Injury Mechanisms in 71 Patients with COVID-19.mSphere. 2020 Jul 15;5(4):e00362-20. doi: 10.1128/mSphere.00362-20. mSphere. 2020. PMID: 32669467 Free PMC article.
-
Clinical and Immune Features of Hospitalized Pediatric Patients With Coronavirus Disease 2019 (COVID-19) in Wuhan, China.JAMA Netw Open. 2020 Jun 1;3(6):e2010895. doi: 10.1001/jamanetworkopen.2020.10895. JAMA Netw Open. 2020. PMID: 32492165 Free PMC article.
-
Immune characteristics of severe and critical COVID-19 patients.Signal Transduct Target Ther. 2020 Aug 31;5(1):179. doi: 10.1038/s41392-020-00296-3. Signal Transduct Target Ther. 2020. PMID: 32868756 Free PMC article. No abstract available.
-
Novel Coronavirus SARS-CoV-2 Target and Disable Natural Killer Cells: Core Immune Effectors for Fighting the Disease.Crit Rev Immunol. 2020;40(2):167-171. doi: 10.1615/CritRevImmunol.2020034441. Crit Rev Immunol. 2020. PMID: 32749094 Review.
-
Immune Parameters and COVID-19 Infection - Associations With Clinical Severity and Disease Prognosis.Front Cell Infect Microbiol. 2020 Jun 30;10:364. doi: 10.3389/fcimb.2020.00364. eCollection 2020. Front Cell Infect Microbiol. 2020. PMID: 32695683 Free PMC article. Review.
Cited by
-
Assessing Predictive Value of SARS-CoV-2 Epitope-Specific CD8+ T-Cell Response in Patients with Severe Symptoms.Vaccines (Basel). 2024 Jun 18;12(6):679. doi: 10.3390/vaccines12060679. Vaccines (Basel). 2024. PMID: 38932408 Free PMC article.
-
Recovery from acute SARS-CoV-2 infection and development of anamnestic immune responses in T cell-depleted rhesus macaques.bioRxiv [Preprint]. 2021 Apr 4:2021.04.02.438262. doi: 10.1101/2021.04.02.438262. bioRxiv. 2021. Update in: mBio. 2021 Aug 31;12(4):e0150321. doi: 10.1128/mBio.01503-21. PMID: 33821272 Free PMC article. Updated. Preprint.
-
Neutrophils and COVID-19: Active Participants and Rational Therapeutic Targets.Front Immunol. 2021 Jun 2;12:680134. doi: 10.3389/fimmu.2021.680134. eCollection 2021. Front Immunol. 2021. PMID: 34149717 Free PMC article. Review.
-
The Role of Aspartate Aminotransferase-to-Lymphocyte Ratio Index (ALRI) in Predicting Mortality in SARS-CoV-2 Infection.Microorganisms. 2023 Nov 30;11(12):2894. doi: 10.3390/microorganisms11122894. Microorganisms. 2023. PMID: 38138038 Free PMC article.
-
Targeting of neutrophil activation in the early phase of the disease for prevention of Coronavirus disease-19 severity.Microbiol Immunol. 2022 Jun;66(6):264-276. doi: 10.1111/1348-0421.12978. Epub 2022 Apr 20. Microbiol Immunol. 2022. PMID: 35348252 Free PMC article. Review.
References
-
- WHO Main Website. https://www.who.int.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
