

Prognostic Value of Interval Between the Initiation of Neoadjuvant Treatment to Surgery for Patients With Locally Advanced Rectal Cancer Following Neoadjuvant Chemotherapy, Radiotherapy and Definitive Surgery
- PMID: 32974129
- PMCID: PMC7473386
- DOI: 10.3389/fonc.2020.01280
Prognostic Value of Interval Between the Initiation of Neoadjuvant Treatment to Surgery for Patients With Locally Advanced Rectal Cancer Following Neoadjuvant Chemotherapy, Radiotherapy and Definitive Surgery
Abstract
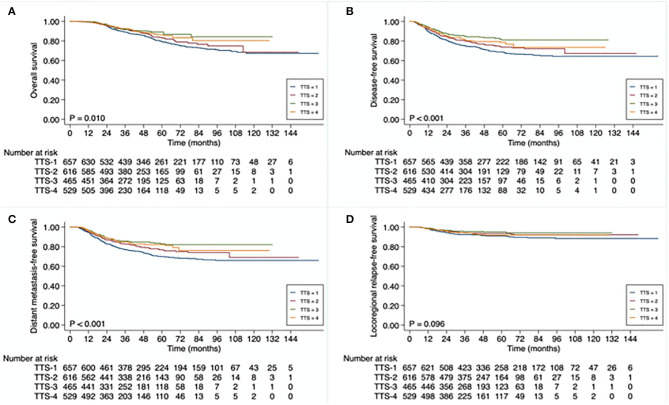
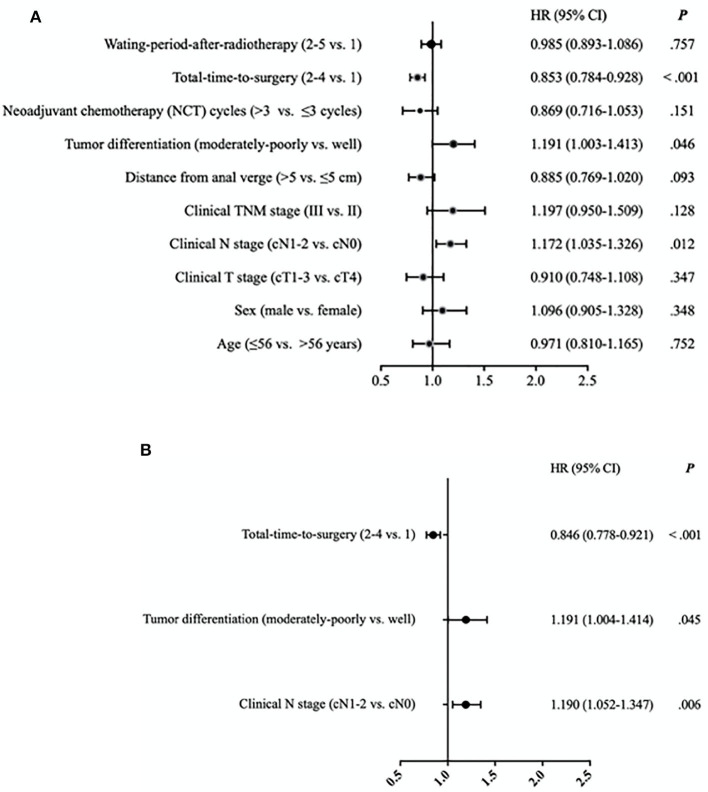
Background: The addition of intensive preoperative chemotherapy and using of a longer waiting period between neoadjuvant radiotherapy and total mesorectal excision (TME) surgery lengthen the time interval from the initiation of neoadjuvant treatment to definitive surgery in patients with locally advanced rectal cancer (LARC). Here, we evaluated the prognostic value of different time intervals between the initiation of neoadjuvant treatment to TME surgery for LARC. Methods: A total of 2,267 patients with LARC, who received neoadjuvant radiochemotherapy and TME surgery, between January 2010 through December 2018 were recruited. The entire cohort was divided into 4 subgroups based on total-time-to surgery, defined as the time interval between initiation of neoadjuvant treatment and TME surgery (TTS): <13 weeks (TTS-1), 13 to <15 weeks (TTS-2), 15 to <17 weeks (TTS-3), ≥17 weeks (TTS-4). Overall survival (OS), disease-free survival (DFS), distant metastasis-free survival (DMFS), and local recurrence-free survival (LRFS) rates in different TTS subgroup patients were compared, and hazard ratios (HR) for different demographic and clinicopathological variables, including TTS, were calculated to determine their prognostic significance. Results: The median follow-up time was 42.0 (range, 5-162) months. The 3-year OS, DFS, DMFS, and LRFS rates were 87.0, 79.4, 80.9, and 93.8%, respectively. The varied OS, DFS, and DFMS rates were detected among these different TTS subgroups (P = 0.010, P < 0.001, and P < 0.001, respectively). Particularly, the lower survival outcome was mainly observed at patients in the shortest TTS group (TTS-1). Cox regression analysis confirmed that the only significant positive independent prognostic factor for 3-year DFS was a longer TTS (TTS 2-4 vs. TTS-1; HR 0.884, 95% CI 0.778-0.921, P < 0.001), while the significant negative independent prognosticfactors were moderate to poor tumor differentiation (vs. well-differentiated; HR 1.191, 95% CI 1.004-1.414, P = 0.045) and clinical N1-2 stage (vs. N0 stage; HR 1.190, 95% CI 1.052-1.347, P = 0.006). Conclusion: For patients with LARC, an interval between the initiation of neoadjuvant treatment and TME surgery of longer than 13 weeks is associated with favorable disease-free survival.
Keywords: locally advanced rectal cancer; neoadjuvant treatment; neoadjuvant treatment interval; prognostic value; surgery interval.
Copyright © 2020 Wan, Zhang, Chen, Liu, Zheng, Lan and He.
Figures
Similar articles
-
[Comparison of long-term efficacy between watch and wait strategy and total mesorectal excision in locally advanced rectal cancer patients with clinical complete response after neoadjuvant therapy].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Mar 25;23(3):266-273. doi: 10.3760/cma.j.cn.441530-20200224-00081. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32192306 Chinese.
-
Timing to achieve the best recurrence-free survival after neoadjuvant chemoradiotherapy in locally advanced rectal cancer: experience in a large-volume center in China.Int J Colorectal Dis. 2021 May;36(5):1007-1016. doi: 10.1007/s00384-020-03829-y. Epub 2021 Jan 4. Int J Colorectal Dis. 2021. PMID: 33398511
-
Tumor deposits: markers of poor prognosis in patients with locally advanced rectal cancer following neoadjuvant chemoradiotherapy.Oncotarget. 2016 Feb 2;7(5):6335-44. doi: 10.18632/oncotarget.6656. Oncotarget. 2016. PMID: 26695441 Free PMC article.
-
Total neoadjuvant therapy or standard chemoradiotherapy for locally advanced rectal cancer: A systematic review and meta-analysis.Front Surg. 2022 Aug 26;9:911538. doi: 10.3389/fsurg.2022.911538. eCollection 2022. Front Surg. 2022. PMID: 36090336 Free PMC article. Review.
-
Interval time between neoadjuvant chemotherapy and surgery in advanced gastric cancer doesn't affect outcome: A meta analysis.Front Surg. 2023 Jan 16;9:1047456. doi: 10.3389/fsurg.2022.1047456. eCollection 2022. Front Surg. 2023. PMID: 36726960 Free PMC article. Review.
Cited by
-
Expression Pattern and Prognostic Value of CTLA-4, CD86, and Tumor-Infiltrating Lymphocytes in Rectal Cancer after Neoadjuvant Chemo(radio)therapy.Cancers (Basel). 2022 Nov 14;14(22):5573. doi: 10.3390/cancers14225573. Cancers (Basel). 2022. PMID: 36428666 Free PMC article.
-
Optimized tools and timing of response reassessment after neoadjuvant chemoradiation in rectal cancer.Int J Colorectal Dis. 2022 Nov;37(11):2321-2333. doi: 10.1007/s00384-022-04268-7. Epub 2022 Oct 15. Int J Colorectal Dis. 2022. PMID: 36243807 Free PMC article.
-
A nomogram for predicting good response after neoadjuvant chemoradiotherapy for locally advanced rectal cancer: a retrospective, double-center, cohort study.Int J Colorectal Dis. 2022 Oct;37(10):2157-2166. doi: 10.1007/s00384-022-04247-y. Epub 2022 Sep 1. Int J Colorectal Dis. 2022. PMID: 36048198 Free PMC article.
References
-
- Benson AB, III, Bekaii-Saab T, Chan E, Chen YJ, Choti MA, Cooper HS, et al. Metastatic colon cancer, version 3.2013: featured updates to the NCCN Guidelines. J Natl Comprehens Cancer Netw. (2013) 11:141–52; quiz 52. - PubMed
-
- van Gijn W, Marijnen CA, Nagtegaal ID, Kranenbarg EM, Putter H, Wiggers T, et al. . Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. (2011) 12:575–82. 10.1016/S1470-2045(11)70097-3 - DOI - PubMed
-
- Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. . Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. (2012) 30:1926–33. 10.1200/JCO.2011.40.1836 - DOI - PubMed
LinkOut - more resources
Full Text Sources