

Diabetic Foot. Part 1: Ulcers and Infections
- PMID: 32968329
- PMCID: PMC7494373
- DOI: 10.1055/s-0039-3402462
Diabetic Foot. Part 1: Ulcers and Infections
Abstract
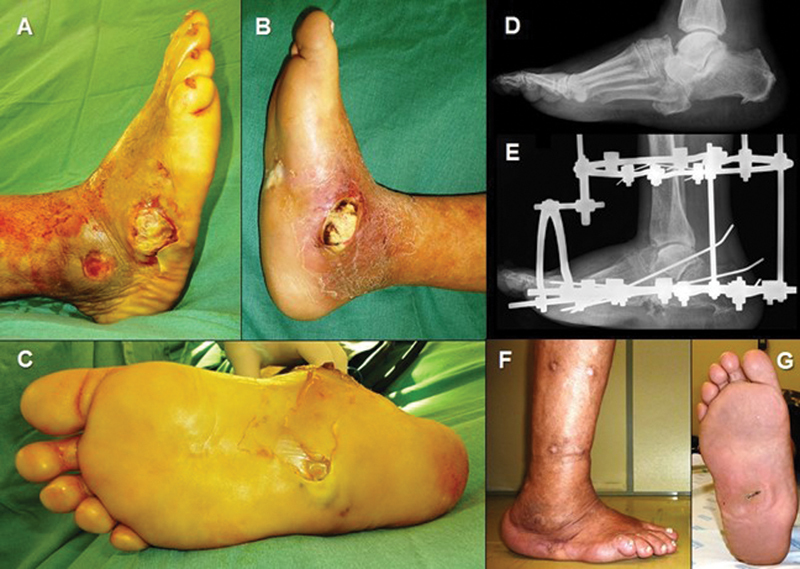
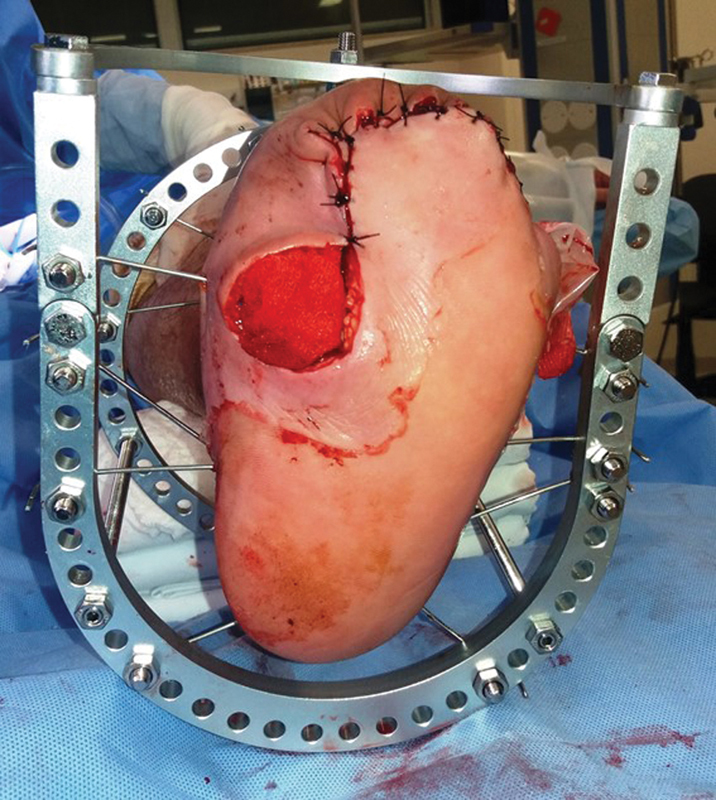
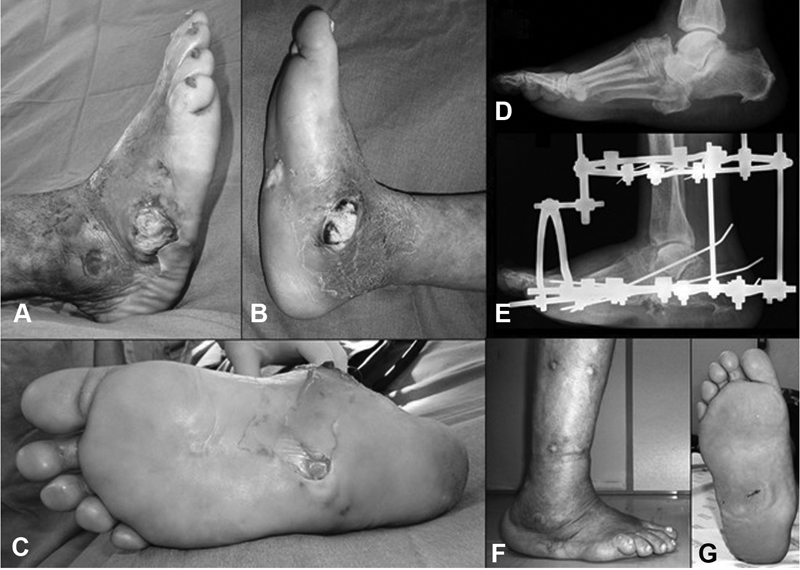
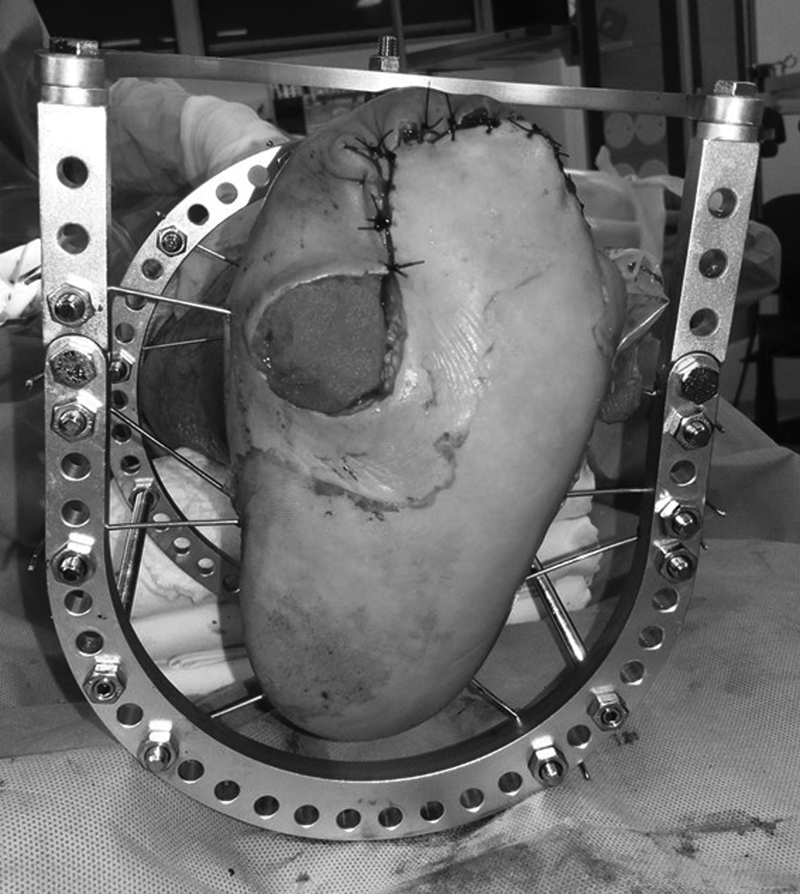
Diabetes is a systemic disease that has achieved epidemic proportions in modern society. Ulcers and infections are common complications in the feet of patients with advanced stages of the disease, and are the main cause of amputation of the lower limb. Peripheral neuropathy is the primary cause of loss of the protective sensation of the feet and frequently leads to plantar pressure ulcers and osteoarticular disruption, which in turn develops into Charcot neuropathy (CN). Common co-factors that add to the morbidity of the disease and the risk of amputation in this population are obesity, peripheral arterial disease, immune and metabolic disorders. Orthopedic surgeons must be aware that the early detection and prevention of these comorbidities, through diligent medical care and patient education, can avoid these amputations.
Keywords: amputation; diabetes; foot; infection; ulcer.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflitos de Interesses O autor declara não haver conflitos de interesses.
Figures
Similar articles
-
Treatment of diabetic foot ulcers.J Cardiovasc Surg (Torino). 2009 Jun;50(3):275-91. J Cardiovasc Surg (Torino). 2009. PMID: 19543189 Review.
-
[Prevention of diabetic foot].Acta Med Croatica. 2013 Oct;67 Suppl 1:35-44. Acta Med Croatica. 2013. PMID: 24371974 Croatian.
-
Outcome after protected full weightbearing treatment in an orthopedic device in diabetic neuropathic arthropathy (Charcot arthropathy): a comparison of unilaterally and bilaterally affected patients.BMC Musculoskelet Disord. 2016 Dec 29;17(1):504. doi: 10.1186/s12891-016-1357-4. BMC Musculoskelet Disord. 2016. PMID: 28031030 Free PMC article.
-
The current burden of diabetic foot disease.J Clin Orthop Trauma. 2021 Feb 8;17:88-93. doi: 10.1016/j.jcot.2021.01.017. eCollection 2021 Jun. J Clin Orthop Trauma. 2021. PMID: 33680841 Free PMC article.
-
Foot ulcers in the diabetic patient, prevention and treatment.Vasc Health Risk Manag. 2007;3(1):65-76. Vasc Health Risk Manag. 2007. PMID: 17583176 Free PMC article. Review.
Cited by
-
Brazilian Society of Angiology and Vascular Surgery 2023 guidelines on the diabetic foot.J Vasc Bras. 2024 May 17;23:e20230087. doi: 10.1590/1677-5449.202300872. eCollection 2024. J Vasc Bras. 2024. PMID: 38803655 Free PMC article.
-
The association between estimated glomerular filtration rate and prognosis in patients with diabetic foot osteomyelitis.Int Wound J. 2022 Nov;19(7):1650-1657. doi: 10.1111/iwj.13765. Epub 2022 Jan 25. Int Wound J. 2022. PMID: 35080116 Free PMC article.
-
Racial and Ethnic Disparities in the Management of Diabetic Feet.Curr Rev Musculoskelet Med. 2023 Nov;16(11):550-556. doi: 10.1007/s12178-023-09867-7. Epub 2023 Sep 21. Curr Rev Musculoskelet Med. 2023. PMID: 37733148 Free PMC article. Review.
-
Bioactive-Glass-Based Materials with Possible Application in Diabetic Wound Healing: A Systematic Review.Int J Mol Sci. 2024 Jan 17;25(2):1152. doi: 10.3390/ijms25021152. Int J Mol Sci. 2024. PMID: 38256225 Free PMC article. Review.
-
Diabetic foot ulcer self-care assessment: a scoping review.Rev Bras Enferm. 2023 Aug 7;76(3):e20220555. doi: 10.1590/0034-7167-2022-0555. eCollection 2023. Rev Bras Enferm. 2023. PMID: 37556696 Free PMC article. Review.
References
-
- Centers for Disease Control and Prevention.National Diabetics Statistics Report 2017 Department of Health and Human Services, Center for Disease Prevention and Control; 2017
-
- Brodsky J W. St Louis, MO: Mosby; 1993. The diabetic foot; pp. 278–283.
-
- Amaral A H, Junior, Amaral L AH, Bastos M G, Nascimento L C, Alves M J, Andrade M AP. Prevenção das lesões de membros inferiores e redução da morbidade em pacientes diabéticos. Rev Bras Ortop. 2014;49(05):482–487. - PubMed
-
- Abbott C A, Carrington A L, Ashe H. The North-West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabet Med. 2002;19(05):377–384. - PubMed
LinkOut - more resources
Full Text Sources