

Risk Factors for Hospitalization, Mechanical Ventilation, or Death Among 10 131 US Veterans With SARS-CoV-2 Infection
- PMID: 32965502
- PMCID: PMC7512055
- DOI: 10.1001/jamanetworkopen.2020.22310
Risk Factors for Hospitalization, Mechanical Ventilation, or Death Among 10 131 US Veterans With SARS-CoV-2 Infection
Abstract
Importance: Identifying independent risk factors for adverse outcomes in patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can support prognostication, resource utilization, and treatment.
Objective: To identify excess risk and risk factors associated with hospitalization, mechanical ventilation, and mortality in patients with SARS-CoV-2 infection.
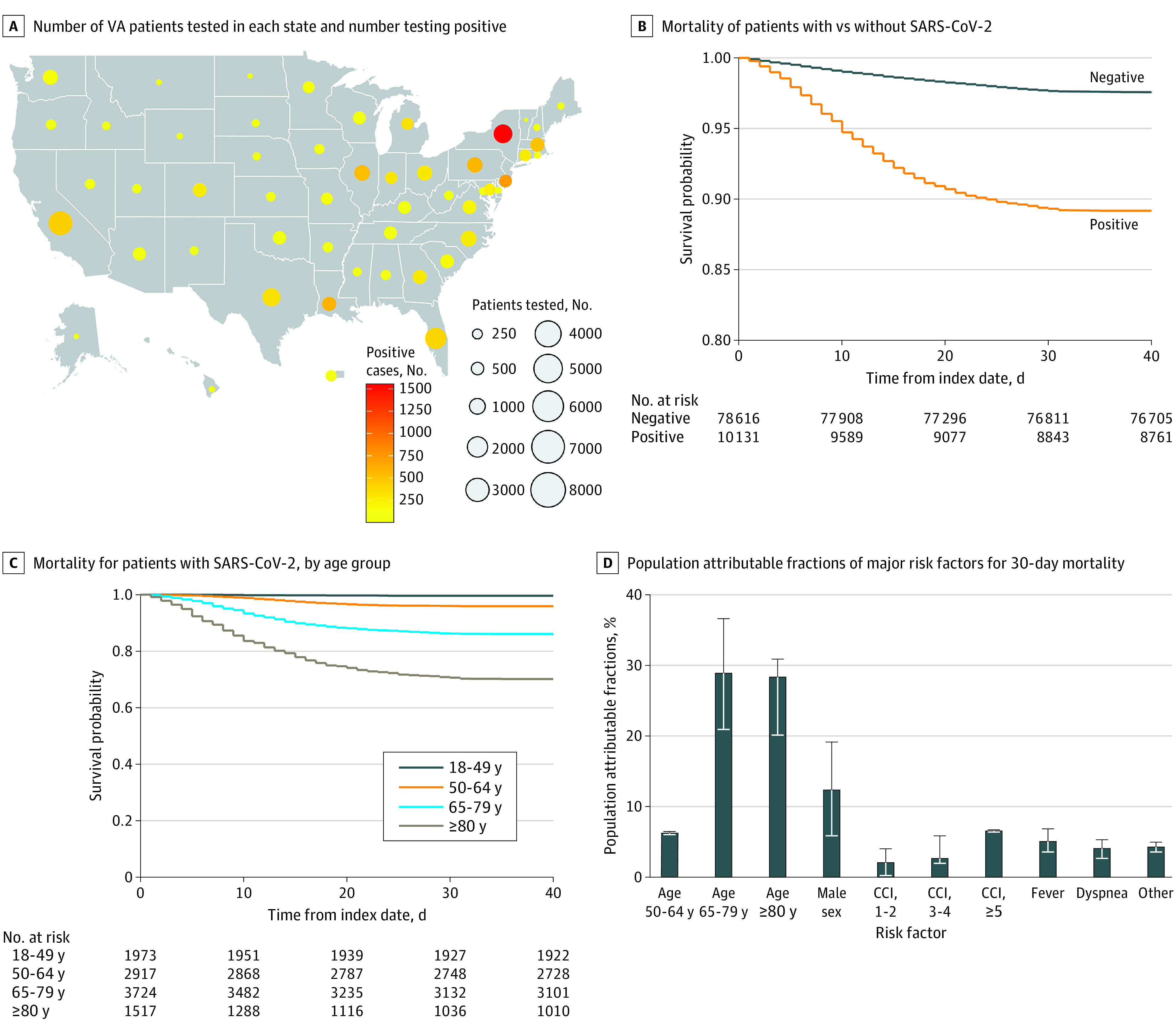
Design, setting, and participants: This longitudinal cohort study included 88 747 patients tested for SARS-CoV-2 nucleic acid by polymerase chain reaction between Feburary 28 and May 14, 2020, and followed up through June 22, 2020, in the Department of Veterans Affairs (VA) national health care system, including 10 131 patients (11.4%) who tested positive.
Exposures: Sociodemographic characteristics, comorbid conditions, symptoms, and laboratory test results.
Main outcomes and measures: Risk of hospitalization, mechanical ventilation, and death were estimated in time-to-event analyses using Cox proportional hazards models.
Results: The 10 131 veterans with SARS-CoV-2 were predominantly male (9221 [91.0%]), with diverse race/ethnicity (5022 [49.6%] White, 4215 [41.6%] Black, and 944 [9.3%] Hispanic) and a mean (SD) age of 63.6 (16.2) years. Compared with patients who tested negative for SARS-CoV-2, those who tested positive had higher rates of 30-day hospitalization (30.4% vs 29.3%; adjusted hazard ratio [aHR], 1.13; 95% CI, 1.08-1.13), mechanical ventilation (6.7% vs 1.7%; aHR, 4.15; 95% CI, 3.74-4.61), and death (10.8% vs 2.4%; aHR, 4.44; 95% CI, 4.07-4.83). Among patients who tested positive for SARS-CoV-2, characteristics significantly associated with mortality included older age (eg, ≥80 years vs <50 years: aHR, 60.80; 95% CI, 29.67-124.61), high regional COVID-19 disease burden (eg, ≥700 vs <130 deaths per 1 million residents: aHR, 1.21; 95% CI, 1.02-1.45), higher Charlson comorbidity index score (eg, ≥5 vs 0: aHR, 1.93; 95% CI, 1.54-2.42), fever (aHR, 1.51; 95% CI, 1.32-1.72), dyspnea (aHR, 1.78; 95% CI, 1.53-2.07), and abnormalities in the certain blood tests, which exhibited dose-response associations with mortality, including aspartate aminotransferase (>89 U/L vs ≤25 U/L: aHR, 1.86; 95% CI, 1.35-2.57), creatinine (>3.80 mg/dL vs 0.98 mg/dL: aHR, 3.79; 95% CI, 2.62-5.48), and neutrophil to lymphocyte ratio (>12.70 vs ≤2.71: aHR, 2.88; 95% CI, 2.12-3.91). With the exception of geographic region, the same covariates were independently associated with mechanical ventilation along with Black race (aHR, 1.52; 95% CI, 1.25-1.85), male sex (aHR, 2.07; 95% CI, 1.30-3.32), diabetes (aHR, 1.40; 95% CI, 1.18-1.67), and hypertension (aHR, 1.30; 95% CI, 1.03-1.64). Notable characteristics that were not significantly associated with mortality in adjusted analyses included obesity (body mass index ≥35 vs 18.5-24.9: aHR, 0.97; 95% CI, 0.77-1.21), Black race (aHR, 1.04; 95% CI, 0.88-1.21), Hispanic ethnicity (aHR, 1.03; 95% CI, 0.79-1.35), chronic obstructive pulmonary disease (aHR, 1.02; 95% CI, 0.88-1.19), hypertension (aHR, 0.95; 95% CI, 0.81-1.12), and smoking (eg, current vs never: aHR, 0.87; 95% CI, 0.67-1.13). Most deaths in this cohort occurred in patients with age of 50 years or older (63.4%), male sex (12.3%), and Charlson Comorbidity Index score of at least 1 (11.1%).
Conclusions and relevance: In this national cohort of VA patients, most SARS-CoV-2 deaths were associated with older age, male sex, and comorbidity burden. Many factors previously reported to be associated with mortality in smaller studies were not confirmed, such as obesity, Black race, Hispanic ethnicity, chronic obstructive pulmonary disease, hypertension, and smoking.
Conflict of interest statement
Figures
Similar articles
-
Association of Race and Ethnicity With Comorbidities and Survival Among Patients With COVID-19 at an Urban Medical Center in New York.JAMA Netw Open. 2020 Sep 1;3(9):e2019795. doi: 10.1001/jamanetworkopen.2020.19795. JAMA Netw Open. 2020. PMID: 32975574 Free PMC article.
-
Risk Factors Associated With SARS-CoV-2 Infections, Hospitalization, and Mortality Among US Nursing Home Residents.JAMA Netw Open. 2021 Mar 1;4(3):e216315. doi: 10.1001/jamanetworkopen.2021.6315. JAMA Netw Open. 2021. PMID: 33787905 Free PMC article.
-
Racial Disparities in Incidence and Outcomes Among Patients With COVID-19.JAMA Netw Open. 2020 Sep 1;3(9):e2021892. doi: 10.1001/jamanetworkopen.2020.21892. JAMA Netw Open. 2020. PMID: 32975575 Free PMC article.
-
Clinical Characteristics and Morbidity Associated With Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit.JAMA Netw Open. 2020 Jun 1;3(6):e2012270. doi: 10.1001/jamanetworkopen.2020.12270. JAMA Netw Open. 2020. PMID: 32543702 Free PMC article. Review.
-
The potential impacts of obesity on COVID-19.Clin Med (Lond). 2020 Jul;20(4):e109-e113. doi: 10.7861/clinmed.2020-0239. Epub 2020 Jun 22. Clin Med (Lond). 2020. PMID: 32571783 Free PMC article. Review.
Cited by
-
A narrative review of COVID-19-related acute respiratory distress syndrome (CARDS): "typical" or "atypical" ARDS?Ann Transl Med. 2022 Aug;10(16):908. doi: 10.21037/atm-22-3717. Ann Transl Med. 2022. PMID: 36111011 Free PMC article. Review.
-
Adverse COVID-19 outcomes in American Veterans with age-related macular degeneration: a case-control study.BMJ Open. 2023 Dec 18;13(12):e071921. doi: 10.1136/bmjopen-2023-071921. BMJ Open. 2023. PMID: 38110385 Free PMC article.
-
Evaluation of risk scores as predictors of mortality and hospital length of stay for older COVID-19 patients.Aging Med (Milton). 2023 Jan 10;6(1):56-62. doi: 10.1002/agm2.12238. eCollection 2023 Mar. Aging Med (Milton). 2023. PMID: 36911090 Free PMC article.
-
The US Department of Veterans Affairs Science and Health Initiative to Combat Infectious and Emerging Life-Threatening Diseases (VA SHIELD): A Biorepository Addressing National Health Threats.Open Forum Infect Dis. 2022 Dec 14;9(12):ofac641. doi: 10.1093/ofid/ofac641. eCollection 2022 Dec. Open Forum Infect Dis. 2022. PMID: 36601554 Free PMC article.
-
Successful Treatment with High-dose Steroids for Acute Exacerbation of Idiopathic Pulmonary Fibrosis Triggered by COVID-19.Intern Med. 2022 Jan 15;61(2):233-236. doi: 10.2169/internalmedicine.8163-21. Epub 2021 Nov 6. Intern Med. 2022. PMID: 34744107 Free PMC article.
References
-
- Herold T, III, Jurinovic V, Arnreich C, et al. . Level of IL-6 predicts respiratory failure in hospitalized symptomatic COVID-19 patients. medRxiv. Preprint published April 10, 2020. doi:10.1101/2020.04.01.20047381 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
