

Randomised clinical trial on 7-days-a-week postoperative radiotherapy vs. concurrent postoperative radio-chemotherapy in locally advanced cancer of the oral cavity/oropharynx
- PMID: 32960662
- PMCID: PMC7716017
- DOI: 10.1259/bjr.20200288
Randomised clinical trial on 7-days-a-week postoperative radiotherapy vs. concurrent postoperative radio-chemotherapy in locally advanced cancer of the oral cavity/oropharynx
Abstract
Objective: To compare the efficacy and tolerance of 7-days-a-week accelerated postoperative radiotherapy (p-CAIR) vs postoperative radio-chemotherapy (p-RTCT).
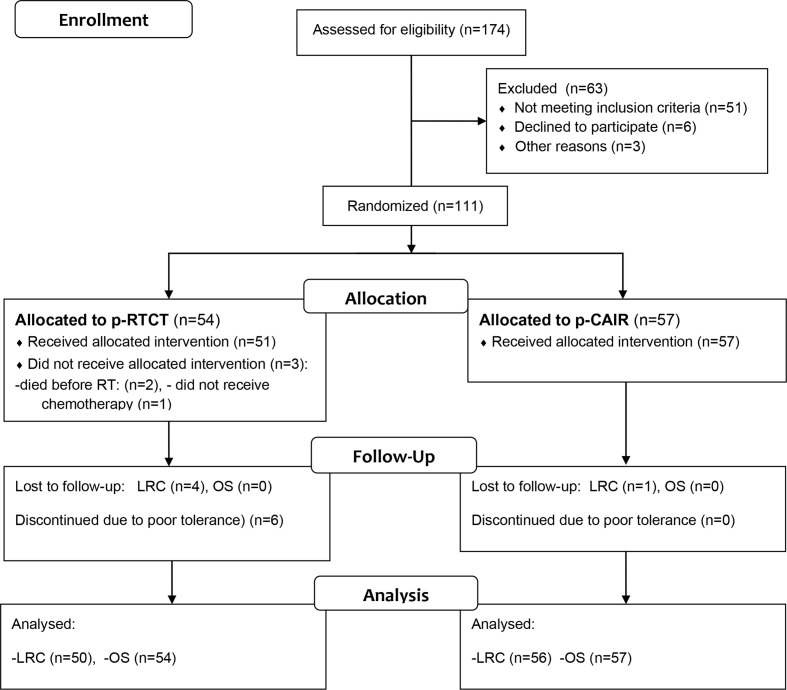
Methods: Between September 2007 and October 2013, 111 patients were enrolled and randomly assigned to receive 63 Gy in 1.8 Gy fractions 7-days-a-week (n = 57, p-CAIR) or 63 Gy in 1.8 Gy fractions 5-days-a-week with concurrent cisplatin 80-100 mg per square meter of body-surface area on days 1, 22 and 43 of the radiotherapy course (p-RTCT). It represents approximately 40% of the intended trial size, that was closed prematurely due to slowing accrual. Only high-risk patients with squamous cell cancer of the oropharynx/oral cavity, considered fit for concurrent treatment were enrolled.
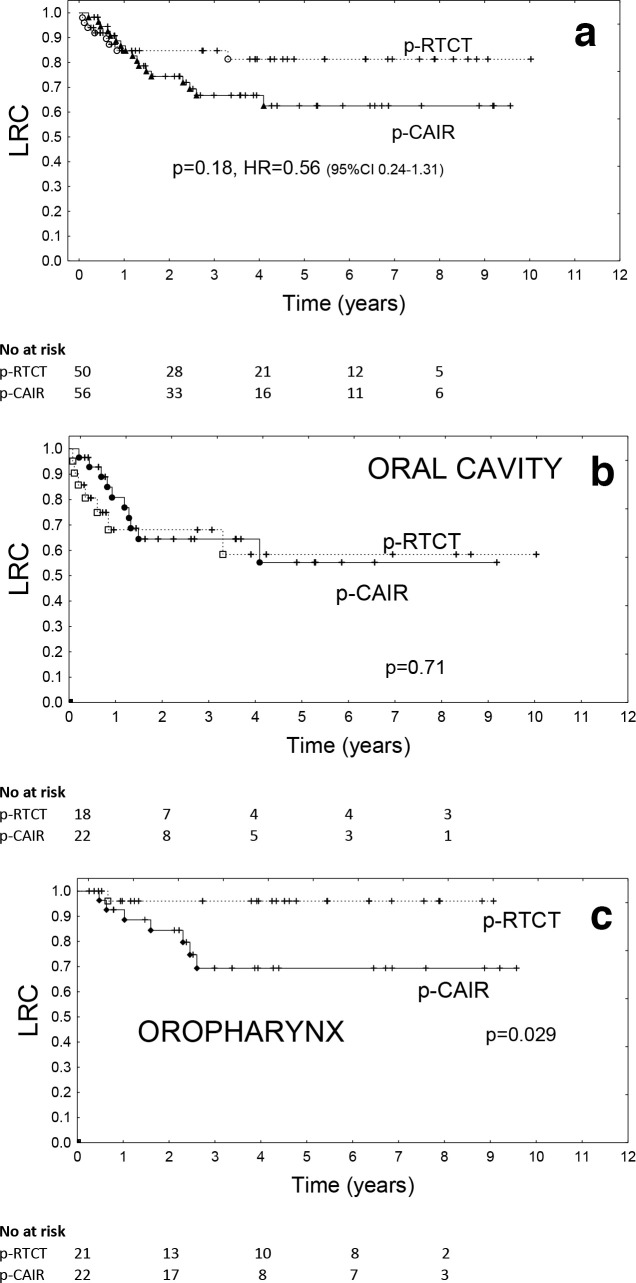
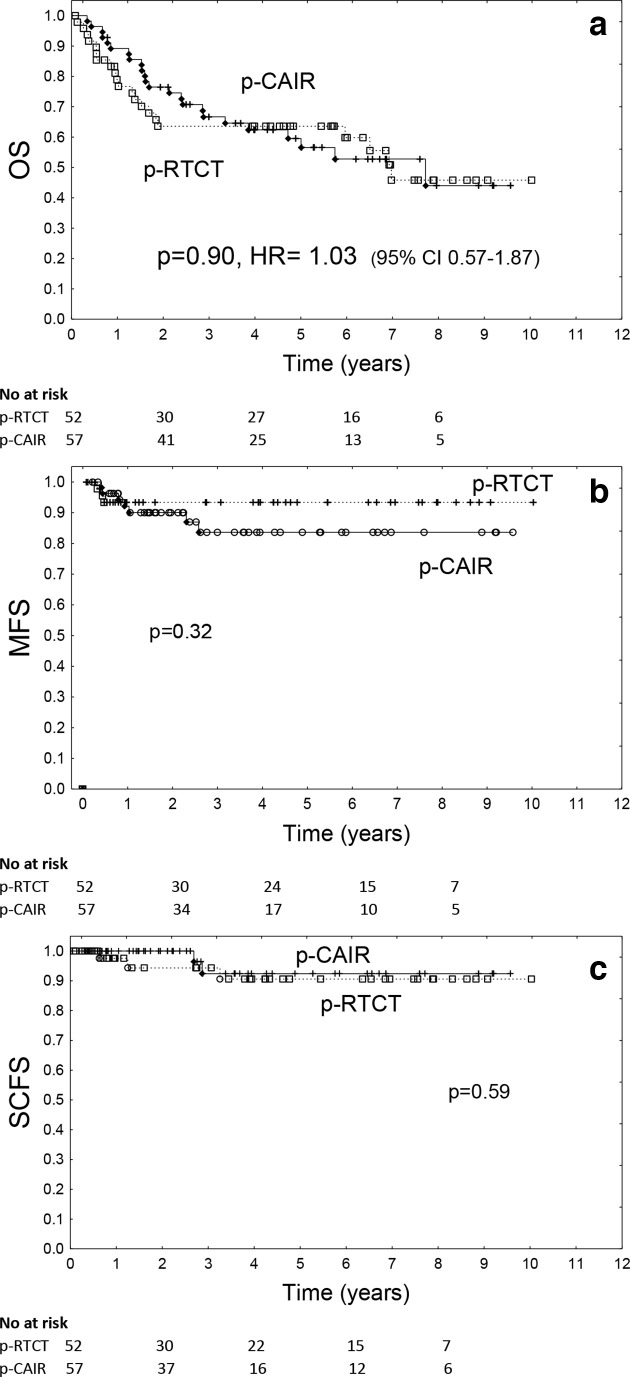
Results: The rate of locoregional control (LRC) did not differ significantly between treatment arms (p = 0.18, HR = 0.56), 5 year LRC tended, however, to favour p-RTCT (81%) vs p-CAIR (62%). There was no difference in overall survival between treatment arms (p = 0.90, HR = 1.03).The incidence and severity of acute mucosal reactions and late reactions did not differ significantly between treatment arms. Haematological toxicity of p-RTCT was, however, considerably increased compared to p-CAIR.
Conclusion: Concurrent postoperative RTCT tended to improve locoregional control rate as compared to p-CAIR. This, however, did not transferred into improved overall survival. Postoperative RTCT was associated with a substantial increase in haematological toxicity that negatively affected treatment compliance in this arm.
Advances in knowledge: To our knowledge, this is the first trial that compares accelerated radiotherapy and radio-chemotherapy in postoperative treatment for oralcavity/oropharyngeal cancer.
Figures

Similar articles
-
Randomized clinical trial on 7-days-a-week post-operative radiotherapy vs concurrent post-operative radiochemotherapy in locally advanced cancer of the oral cavity/oropharynx: a report on acute normal tissue reactions.Br J Radiol. 2016;89(1061):20150805. doi: 10.1259/bjr.20150805. Epub 2016 Mar 2. Br J Radiol. 2016. PMID: 26934504 Free PMC article. Clinical Trial.
-
Randomized clinical trial on 7-days-a-week postoperative radiotherapy for high-risk squamous cell head and neck cancer.Radiother Oncol. 2008 May;87(2):155-63. doi: 10.1016/j.radonc.2008.02.009. Epub 2008 Mar 14. Radiother Oncol. 2008. PMID: 18342964 Clinical Trial.
-
Preoperative induction chemotherapy followed by concurrent chemoradiotherapy in advanced carcinoma of the oral cavity and oropharynx.Cancer. 2000 Sep 1;89(5):939-45. doi: 10.1002/1097-0142(20000901)89:5<939::aid-cncr1>3.0.co;2-6. Cancer. 2000. PMID: 10964322 Clinical Trial.
-
Interventions for the treatment of oral cavity and oropharyngeal cancer: chemotherapy.Cochrane Database Syst Rev. 2010 Sep 8;(9):CD006386. doi: 10.1002/14651858.CD006386.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2011 Apr 13;(4):CD006386. doi: 10.1002/14651858.CD006386.pub3 PMID: 20824847 Updated. Review.
-
Interventions for the treatment of oral cavity and oropharyngeal cancer: chemotherapy.Cochrane Database Syst Rev. 2011 Apr 13;(4):CD006386. doi: 10.1002/14651858.CD006386.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2021 Dec 20;12:CD006386. doi: 10.1002/14651858.CD006386.pub4 PMID: 21491393 Updated. Review.
References
-
- Awwad HK, Lotayef M, Shouman T, Begg AC, Wilson G, Bentzen SM, et al. . Accelerated hyperfractionation (AHF) compared to conventional fractionation (CF) in the postoperative radiotherapy of locally advanced head and neck cancer: influence of proliferation. Br J Cancer 2002; 86: 517–23. doi: 10.1038/sj.bjc.6600119 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
