

Projections of incident atherosclerotic cardiovascular disease and incident type 2 diabetes across evolving statin treatment guidelines and recommendations: A modelling study
- PMID: 32845900
- PMCID: PMC7449387
- DOI: 10.1371/journal.pmed.1003280
Projections of incident atherosclerotic cardiovascular disease and incident type 2 diabetes across evolving statin treatment guidelines and recommendations: A modelling study
Abstract
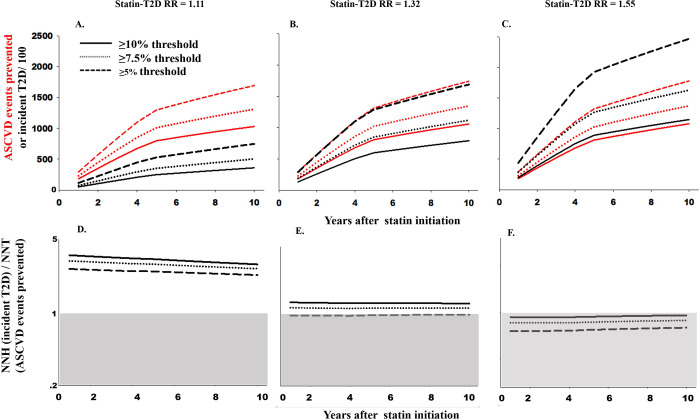
Background: Experimental and observational research has suggested the potential for increased type 2 diabetes (T2D) risk among populations taking statins for the primary prevention of atherosclerotic cardiovascular disease (ASCVD). However, few studies have directly compared statin-associated benefits and harms or examined heterogeneity by population subgroups or assumed treatment effect. Thus, we compared ASCVD risk reduction and T2D incidence increases across 3 statin treatment guidelines or recommendations among adults without a history of ASCVD or T2D who were eligible for statin treatment initiation.
Methods and findings: Simulations were conducted using Markov models that integrated data from contemporary population-based studies of non-Hispanic African American and white adults aged 40-75 years with published meta-analyses. Statin treatment eligibility was determined by predicted 10-year ASCVD risk (5%, 7.5%, or 10%). We calculated the number needed to treat (NNT) to prevent one ASCVD event and the number needed to harm (NNH) to incur one incident case of T2D. The likelihood to be helped or harmed (LHH) was calculated as ratio of NNH to NNT. Heterogeneity in statin-associated benefit was examined by sex, age, and statin-associated T2D relative risk (RR) (range: 1.11-1.55). A total of 61,125,042 U.S. adults (58.5% female; 89.4% white; mean age = 54.7 years) composed our primary prevention population, among whom 13-28 million adults were eligible for statin initiation. Overall, the number of ASCVD events prevented was at least twice as large as the number of incident cases of T2D incurred (LHH range: 2.26-2.90). However, the number of T2D cases incurred surpassed the number of ASCVD events prevented when higher statin-associated T2D RRs were assumed (LHH range: 0.72-0.94). In addition, females (LHH range: 1.74-2.40) and adults aged 40-50 years (LHH range: 1.00-1.14) received lower absolute benefits of statin treatment compared with males (LHH range: 2.55-3.00) and adults aged 70-75 years (LHH range: 3.95-3.96). Projected differences in LHH by age and sex became more pronounced as statin-associated T2D RR increased, with a majority of scenarios projecting LHHs < 1 for females and adults aged 40-50 years. This study's primary limitation was uncertainty in estimates of statin-associated T2D risk, highlighting areas in which additional clinical and public health research is needed.
Conclusions: Our projections suggest that females and younger adult populations shoulder the highest relative burden of statin-associated T2D risk.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Utility of Nontraditional Risk Markers in Individuals Ineligible for Statin Therapy According to the 2013 American College of Cardiology/American Heart Association Cholesterol Guidelines.Circulation. 2015 Sep 8;132(10):916-22. doi: 10.1161/CIRCULATIONAHA.115.016846. Epub 2015 Jul 29. Circulation. 2015. PMID: 26224808 Free PMC article.
-
Implications of the new American College of Cardiology/American Heart Association cholesterol guidelines for primary atherosclerotic cardiovascular disease event prevention in a multi ethnic cohort: Multi-Ethnic Study of Atherosclerosis (MESA).Am Heart J. 2015 Mar;169(3):387-395.e3. doi: 10.1016/j.ahj.2014.12.018. Epub 2015 Jan 6. Am Heart J. 2015. PMID: 25728729 Free PMC article.
-
Impact of the 2013 Cholesterol Guideline on Patterns of Lipid-Lowering Treatment in Patients with Atherosclerotic Cardiovascular Disease or Diabetes After 1 Year.J Manag Care Spec Pharm. 2016 Aug;22(8):901-8. doi: 10.18553/jmcp.2016.22.8.901. J Manag Care Spec Pharm. 2016. PMID: 27459652 Free PMC article.
-
The use of statins in people at risk of developing diabetes mellitus: evidence and guidance for clinical practice.Atheroscler Suppl. 2014 Jun;15(1):1-15. doi: 10.1016/j.atherosclerosissup.2014.04.001. Atheroscler Suppl. 2014. PMID: 24840509 Review.
-
Clinical assessment of lurasidone benefit and risk in the treatment of bipolar I depression using number needed to treat, number needed to harm, and likelihood to be helped or harmed.J Affect Disord. 2014 Feb;155:20-7. doi: 10.1016/j.jad.2013.10.040. Epub 2013 Oct 28. J Affect Disord. 2014. PMID: 24246116 Review.
Cited by
-
Bisphosphonate Use and Risk of Atypical Femoral Fractures: A Danish Case-Cohort Study With Blinded Radiographic Review.J Clin Endocrinol Metab. 2024 Oct 15;109(11):e2141-e2150. doi: 10.1210/clinem/dgae023. J Clin Endocrinol Metab. 2024. PMID: 38198798 Free PMC article.
References
-
- Gu Q, Paulose-Ram R, Burt V, Kit B. Prescription cholesterol-lowering medication use in adults aged 40 and over: United States, 2003–2012 NCHS data brief, no 177. Hyattsville, MD: National Center for Health Statistics, US Department of Health and Human Services, CDC; 2014. 2015. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2014;63(25 Pt B):2889–934. 10.1016/j.jacc.2013.11.002 - DOI - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2019;73(24):e285–e350. 10.1016/j.jacc.2018.11.003 - DOI - PubMed
-
- National Cholesterol Education Program Expert Panel on Detection E, Treatment of High Blood Cholesterol in A. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–421. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
