

Pharmacology of Pulmonary Arterial Hypertension: An Overview of Current and Emerging Therapies
- PMID: 32832865
- PMCID: PMC7432664
- DOI: 10.1021/acsptsci.0c00048
Pharmacology of Pulmonary Arterial Hypertension: An Overview of Current and Emerging Therapies
Abstract
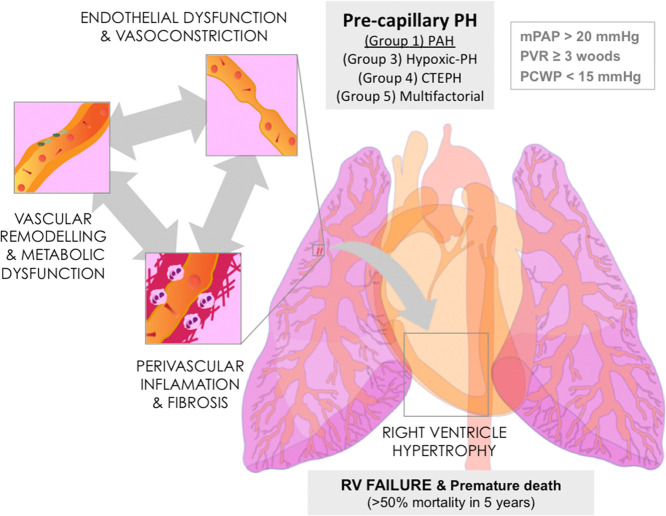
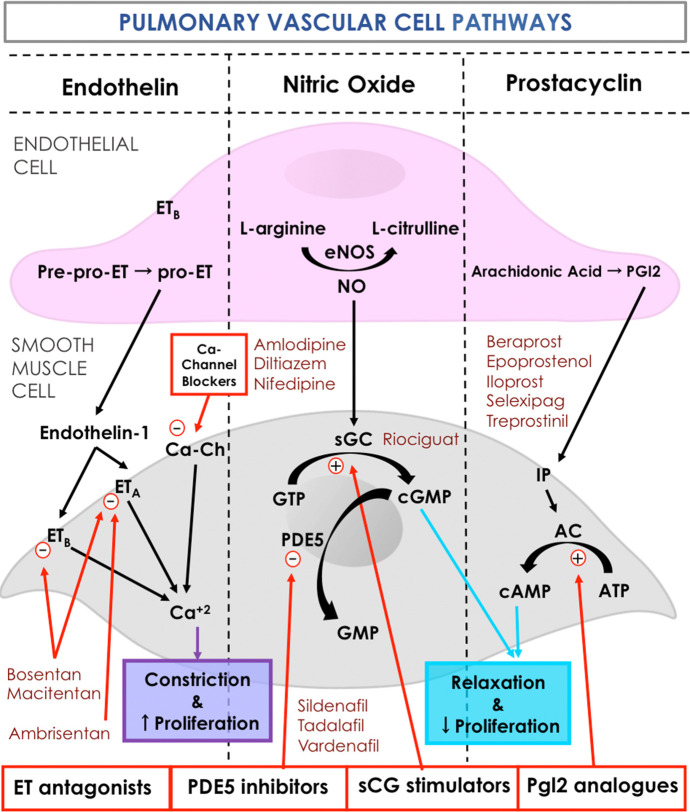
Pulmonary arterial hypertension is a rare and devastating disease characterized by an abnormal chronic increase in pulmonary arterial pressure above 20 mmHg at rest, with a poor prognosis if not treated. Currently, there is not a single fully effective therapy, even though a dozen of drugs have been developed in the last decades. Pulmonary arterial hypertension is a multifactorial disease, meaning that several molecular mechanisms are implicated in its pathology. The main molecular pathways regulating the pulmonary vasomotor tone-endothelin, nitric oxide, and prostacyclin-are the most biologically and therapeutically explored to date. However, drugs targeting these pathways have already found their limitations. In the last years, translational research and clinical trials have made a strong effort in suggesting and testing novel therapeutic strategies for this disease. These approaches involve targeting the main molecular pathways with novel drugs, drug repurposing for novel targets, and also using combinatorial therapies. In this review, we summarize current strategies and drugs targeting the endothelin, nitric oxide, and prostacyclin pathways, as well as, the emerging new drugs proposed to cope with vascular remodelling, metabolic switch, perivascular inflammation, epigenetic modifications, estrogen deregulation, serotonin, and other neurohumoral mechanisms characteristic of this disease. Nowadays, pulmonary arterial hypertension remains an incurable disease; however, the incoming new knowledge makes us believe that new promising therapies are coming to the clinical arena soon.
Copyright © 2020 American Chemical Society.
Conflict of interest statement
The authors declare no competing financial interest.
Figures
Similar articles
-
Transcription factors and potential therapeutic targets for pulmonary hypertension.Front Cell Dev Biol. 2023 Mar 17;11:1132060. doi: 10.3389/fcell.2023.1132060. eCollection 2023. Front Cell Dev Biol. 2023. PMID: 37009479 Free PMC article. Review.
-
Strategizing Drug Therapies in Pulmonary Hypertension for Improved Outcomes.Pharmaceuticals (Basel). 2022 Oct 10;15(10):1242. doi: 10.3390/ph15101242. Pharmaceuticals (Basel). 2022. PMID: 36297354 Free PMC article. Review.
-
Pulmonary arterial hypertension: new insights into the optimal role of current and emerging prostacyclin therapies.Am J Cardiol. 2013 Mar 4;111(5 Suppl):1A-16A; quiz 17A-19A. doi: 10.1016/j.amjcard.2012.12.002. Am J Cardiol. 2013. PMID: 23414683 Review.
-
Medical therapies for pulmonary arterial hypertension.Heart Fail Rev. 2016 May;21(3):273-83. doi: 10.1007/s10741-016-9527-x. Heart Fail Rev. 2016. PMID: 26791159 Review.
-
A Review of Targeted Pulmonary Arterial Hypertension-Specific Pharmacotherapy.J Clin Med. 2016 Dec 6;5(12):114. doi: 10.3390/jcm5120114. J Clin Med. 2016. PMID: 27929408 Free PMC article. Review.
Cited by
-
Multifunctional nanoparticle-mediated combining therapy for human diseases.Signal Transduct Target Ther. 2024 Jan 1;9(1):1. doi: 10.1038/s41392-023-01668-1. Signal Transduct Target Ther. 2024. PMID: 38161204 Free PMC article. Review.
-
Effect of Coronavirus Disease 2019 in Pulmonary Circulation. The Particular Scenario of Precapillary Pulmonary Hypertension.Diagnostics (Basel). 2020 Jul 31;10(8):548. doi: 10.3390/diagnostics10080548. Diagnostics (Basel). 2020. PMID: 32752129 Free PMC article. Review.
-
The Relevance of the Endothelium in Cardiopulmonary Disorders.Int J Mol Sci. 2024 Aug 27;25(17):9260. doi: 10.3390/ijms25179260. Int J Mol Sci. 2024. PMID: 39273209 Free PMC article. Review.
-
Novel Pyrazolo[3,4-b] Pyridine Derivative (HLQ2g) Attenuates Hypoxic Pulmonary Hypertension via Restoring cGKI Expression and BMP Signaling Pathway.Front Pharmacol. 2021 Oct 1;12:691405. doi: 10.3389/fphar.2021.691405. eCollection 2021. Front Pharmacol. 2021. PMID: 34658848 Free PMC article.
-
Therapeutic approaches for pulmonary hypertension in patients with chronic kidney disease.Curr Opin Nephrol Hypertens. 2024 Sep 1;33(5):494-502. doi: 10.1097/MNH.0000000000001008. Epub 2024 Jun 19. Curr Opin Nephrol Hypertens. 2024. PMID: 38899951 Review.
References
-
- Galie N.; Humbert M.; Vachiery J.-L.; Gibbs S.; Lang I.; Torbicki A.; Simonneau G.; Peacock A.; Vonk Noordegraaf A.; Beghetti M.; Ghofrani A.; Gomez Sanchez M. A.; Hansmann G.; Klepetko W.; Lancellotti P.; Matucci M.; McDonagh T.; Pierard L. A.; Trindade P. T.; Zompatori M.; Hoeper M. (2016) 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 37 (1), 67.10.1093/eurheartj/ehv317. - DOI - PubMed
-
- Wijeratne D. T.; Lajkosz K.; Brogly S. B.; Lougheed M. D.; Jiang L.; Housin A.; Barber D.; Johnson A.; Doliszny K. M.; Archer S. L. (2018) Increasing Incidence and Prevalence of World Health Organization Groups 1 to 4 Pulmonary Hypertension: A Population-Based Cohort Study in Ontario, Canada.. Circ Cardiovasc Qual Outcomes 11 (2), e00397310.1161/CIRCOUTCOMES.117.003973. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources