

Cost-effectiveness of the PDSAFE personalised physiotherapy intervention for fall prevention in Parkinson's: an economic evaluation alongside a randomised controlled trial
- PMID: 32781987
- PMCID: PMC7418432
- DOI: 10.1186/s12883-020-01852-8
Cost-effectiveness of the PDSAFE personalised physiotherapy intervention for fall prevention in Parkinson's: an economic evaluation alongside a randomised controlled trial
Abstract
Background: PDSAFE is an individually-tailored, physiotherapist-delivered, balance, strength and strategy training programme aimed at preventing falls among people with Parkinson's. We evaluated the cost-effectiveness of PDSAFE compared with usual care for people with Parkinson's at higher risk of falling, from a UK National Health Service and Personal Social Service perspective.
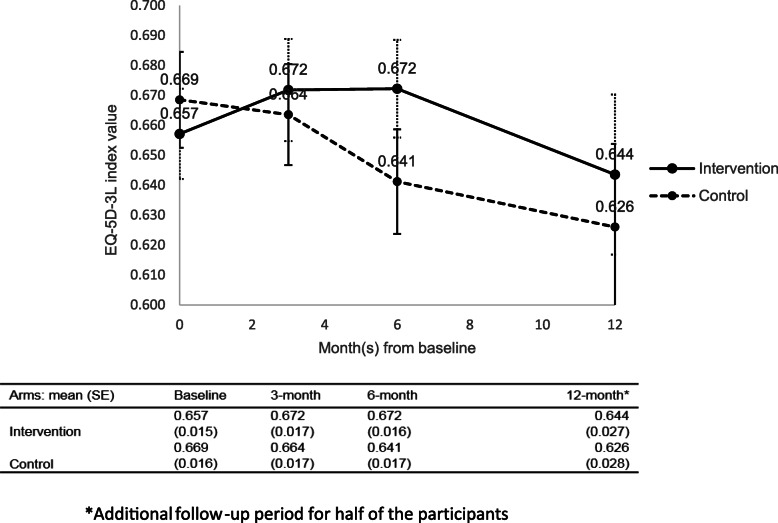
Methods: Resource use and quality of life data (EQ-5D-3L) were collected from 238 participants randomised to the PDSAFE intervention and 236 participants randomised to control, at baseline, 3 months, 6 months (primary outcome), and 12 months. Adjusted cost and quality-adjusted life-years (QALYs) were estimated using generalised linear models and uncertainty estimated using a non-parametric bootstrap.
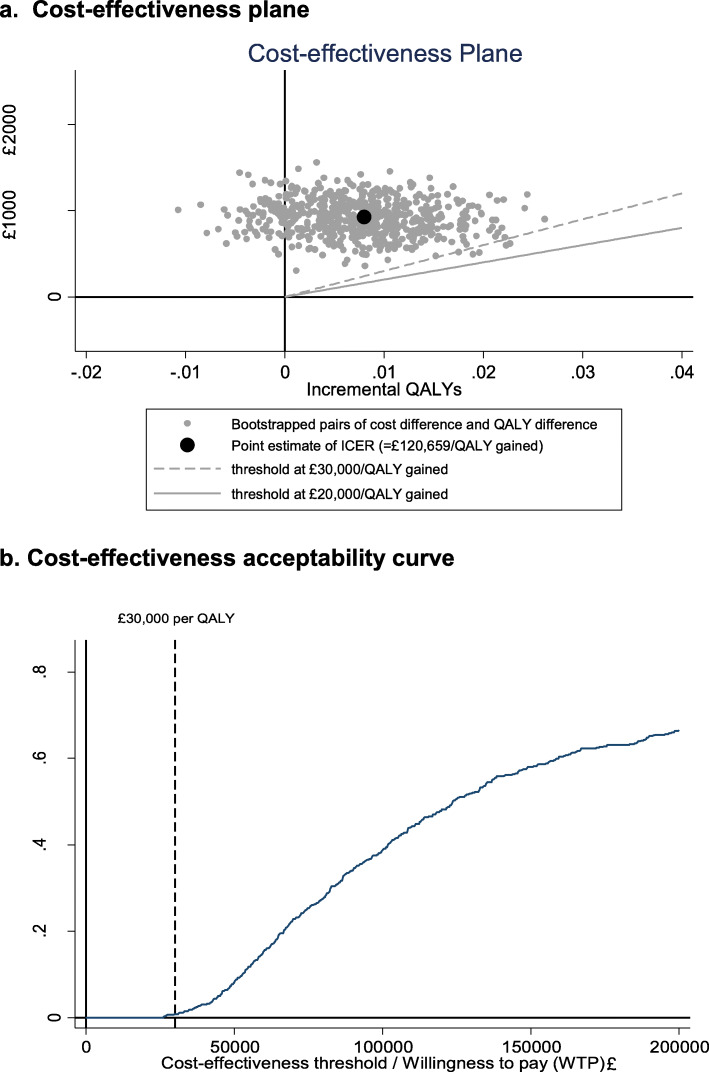
Results: Over 6 months, the PDSAFE intervention was associated with an incremental cost of £925 (95% CI £428 to £1422) and a very small and statistically insignificant QALY gain of 0.008 (95% CI - 0.006 to 0.021). The resulting incremental cost-effectiveness ratio (ICER) was £120,659 per QALY and the probability of the intervention being cost-effective at a UK threshold of £30,000/QALY was less than 1%. The ICER varied substantially across subgroups although no subgroup had an ICER lower than the £30,000 threshold. The result was sensitive to the time horizon with the ICER reducing to £55,176 per QALY when adopting a 12-month time horizon and assuming a sustained treatment effect on QoL, nevertheless, the intervention was still not cost-effective according to the current UK threshold.
Conclusions: Evidence from this trial suggests that the PDSAFE intervention is unlikely to be cost-effective at 6 months. The 12-month analysis suggested that the intervention became closer to being cost-effective if quality of life effects were sustained beyond the intervention period, however this would require confirmation. Further research, including qualitative studies, should be conducted to better understand the treatment effect of physiotherapy and its impact on quality of life in people with Parkinson's given existing mixed evidence on this topic.
Trial registration: ISRCTN48152791. Registered 17 April 2014. http://www.isrctn.com/ISRCTN48152791.
Keywords: Cost; Cost-effectiveness; Parkinson’s; Physiotherapist; Quality of life.
Conflict of interest statement
Dr. Goodwin reports grants from National Institute for Health Research, during the conduct of the study. Prof. Lamb reports grants from NIHR Health technology Assessment Programme during the conduct of this study. Prof. Lamb was a member of the HTA Additional Capacity Funding Board, HTA End of Life Care and Add-on Studies, HTA Prioritisation Group, HTA Trauma Board during this study. Prof. McIntosh is a member of the NIHR Public Health Research Funding board. All other authors have nothing to disclose.
Figures
Similar articles
-
Exercise- and strategy-based physiotherapy-delivered intervention for preventing repeat falls in people with Parkinson's: the PDSAFE RCT.Health Technol Assess. 2019 Jul;23(36):1-150. doi: 10.3310/hta23360. Health Technol Assess. 2019. PMID: 31339100 Free PMC article. Clinical Trial.
-
Multicentre, randomised controlled trial of PDSAFE, a physiotherapist-delivered fall prevention programme for people with Parkinson's.J Neurol Neurosurg Psychiatry. 2019 Jul;90(7):774-782. doi: 10.1136/jnnp-2018-319448. Epub 2019 Apr 3. J Neurol Neurosurg Psychiatry. 2019. PMID: 30944149 Free PMC article. Clinical Trial.
-
A multi-centre, randomised controlled trial of the effectiveness of PDSAFE to prevent falls among people with Parkinson's: study protocol.BMC Neurol. 2015 May 15;15:81. doi: 10.1186/s12883-015-0332-2. BMC Neurol. 2015. PMID: 25971244 Free PMC article. Clinical Trial.
-
"Staying safe" - a narrative review of falls prevention in people with Parkinson's - "PDSAFE".Disabil Rehabil. 2019 Oct;41(21):2596-2605. doi: 10.1080/09638288.2018.1471167. Epub 2018 May 18. Disabil Rehabil. 2019. PMID: 29774765 Review.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.Health Technol Assess. 2006 Mar;10(9):1-132. iii-iv. doi: 10.3310/hta10090. Health Technol Assess. 2006. PMID: 16545208 Review.
Cited by
-
Health-related quality of life in Parkinson's disease: systematic review and meta-analysis of EuroQol (EQ-5D) utility scores.Qual Life Res. 2024 Jul;33(7):1781-1793. doi: 10.1007/s11136-024-03646-8. Epub 2024 Apr 6. Qual Life Res. 2024. PMID: 38581635 Review.
-
A single-blind, randomised control trial on the effectiveness of a structured multi component training module for family caregiver of persons with Parkinson's disease: A study protocol.PLoS One. 2024 Nov 11;19(11):e0309648. doi: 10.1371/journal.pone.0309648. eCollection 2024. PLoS One. 2024. PMID: 39527590 Free PMC article. Clinical Trial.
-
Cost-Effectiveness Analyses of Non-Pharmacological and Non-Surgical Interventions in Idiopathic Parkinson's Disease: A Systematic Review.J Parkinsons Dis. 2024;14(s1):S241-S252. doi: 10.3233/JPD-230213. J Parkinsons Dis. 2024. PMID: 38339939 Free PMC article.
-
Interventions for preventing falls in Parkinson's disease.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD011574. doi: 10.1002/14651858.CD011574.pub2. Cochrane Database Syst Rev. 2022. PMID: 35665915 Free PMC article. Review.
References
-
- Partridge N, Scadding J. The James Lind Alliance: patients and clinicians should jointly identify their priorities for clinical trials. Lancet. 2004;364(9449):1923–1924. - PubMed
-
- Thurman DJ, Stevens JA, Rao JK. Practice parameter: assessing patients in a neurology practice for risk of falls (an evidence-based review): report of the quality standards Subcommittee of the American Academy of neurology. Neurology. 2008;70(6):473–479. - PubMed
-
- Genever RW, Downes TW, Medcalf P. Fracture rates in Parkinson's disease compared with age- and gender-matched controls: a retrospective cohort study. Age Ageing. 2005;34(1):21–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
