

Inferred duration of infectious period of SARS-CoV-2: rapid scoping review and analysis of available evidence for asymptomatic and symptomatic COVID-19 cases
- PMID: 32759252
- PMCID: PMC7409948
- DOI: 10.1136/bmjopen-2020-039856
Inferred duration of infectious period of SARS-CoV-2: rapid scoping review and analysis of available evidence for asymptomatic and symptomatic COVID-19 cases
Abstract
Objectives: Our objective was to review the literature on the inferred duration of the infectious period of COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, and provide an overview of the variation depending on the methodological approach.
Design: Rapid scoping review. Literature review with fixed search terms, up to 1 April 2020. Central tendency and variation of the parameter estimates for infectious period in (A) asymptomatic and (B) symptomatic cases from (1) virological studies (repeated testing), (2) tracing studies and (3) modelling studies were gathered. Narrative review of viral dynamics.
Information sources: Search strategies developed and the following searched: PubMed, Google Scholar, MedRxiv and BioRxiv. Additionally, the Health Information Quality Authority (Ireland) viral load synthesis was used, which screened literature from PubMed, Embase, ScienceDirect, NHS evidence, Cochrane, medRxiv and bioRxiv, and HRB open databases.
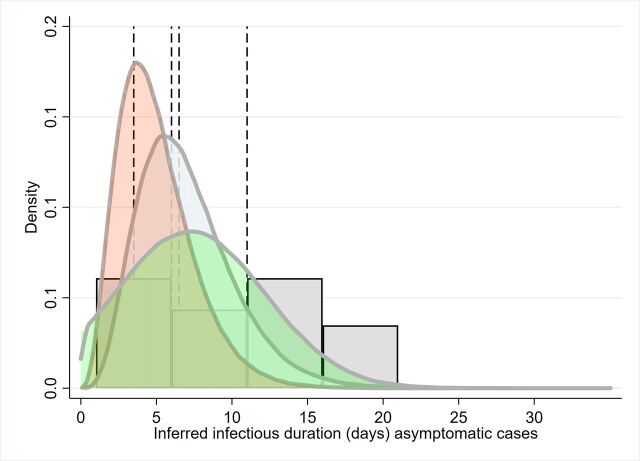
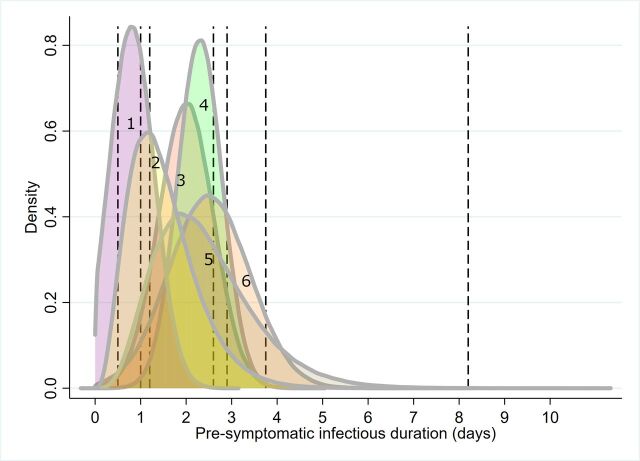
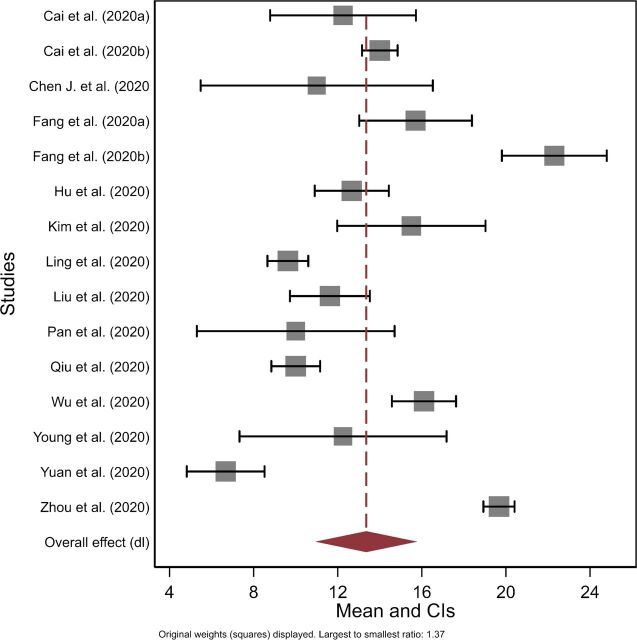
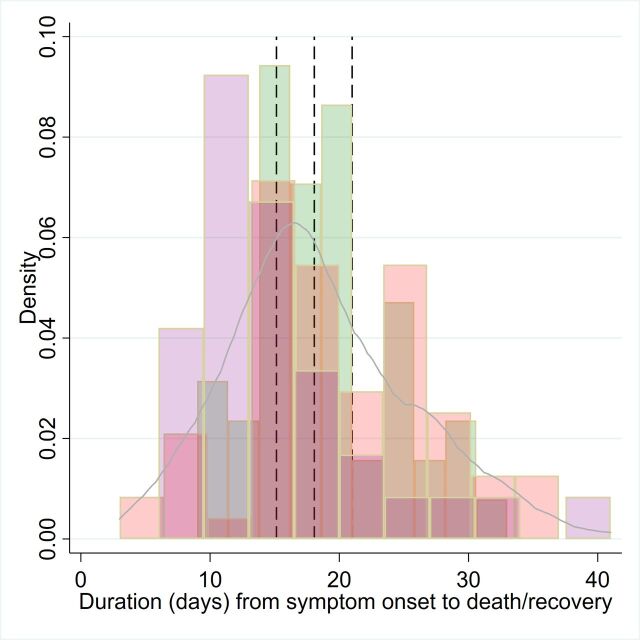
Results: There was substantial variation in the estimates, and how infectious period was inferred. One study provided approximate median infectious period for asymptomatic cases of 6.5-9.5 days. Median presymptomatic infectious period across studies varied over <1-4 days. Estimated mean time from symptom onset to two negative RT-PCR tests was 13.4 days (95% CI 10.9 to 15.8) but was shorter when studies included children or less severe cases. Estimated mean duration from symptom onset to hospital discharge or death (potential maximal infectious period) was 18.1 days (95% CI 15.1 to 21.0); time to discharge was on average 4 days shorter than time to death. Viral dynamic data and model infectious parameters were often shorter than repeated diagnostic data.
Conclusions: There are limitations of inferring infectiousness from repeated diagnosis, viral loads and viral replication data alone and also potential patient recall bias relevant to estimating exposure and symptom onset times. Despite this, available data provide a preliminary evidence base to inform models of central tendency for key parameters and variation for exploring parameter space and sensitivity analysis.
Keywords: epidemiology; infectious diseases; public health; virology.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2022 Jul 22;7(7):CD013705. doi: 10.1002/14651858.CD013705.pub3. Cochrane Database Syst Rev. 2022. PMID: 35866452 Free PMC article. Review.
-
Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis.PLoS Med. 2020 Sep 22;17(9):e1003346. doi: 10.1371/journal.pmed.1003346. eCollection 2020 Sep. PLoS Med. 2020. PMID: 32960881 Free PMC article.
-
Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility.N Engl J Med. 2020 May 28;382(22):2081-2090. doi: 10.1056/NEJMoa2008457. Epub 2020 Apr 24. N Engl J Med. 2020. PMID: 32329971 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease.Cochrane Database Syst Rev. 2020 Jul 7;7(7):CD013665. doi: 10.1002/14651858.CD013665. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Feb 23;2:CD013665. doi: 10.1002/14651858.CD013665.pub2 PMID: 32633856 Free PMC article. Updated.
-
Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review.JAMA. 2020 Aug 25;324(8):782-793. doi: 10.1001/jama.2020.12839. JAMA. 2020. PMID: 32648899 Review.
Cited by
-
Risk of rapid evolutionary escape from biomedical interventions targeting SARS-CoV-2 spike protein.PLoS One. 2021 Apr 28;16(4):e0250780. doi: 10.1371/journal.pone.0250780. eCollection 2021. PLoS One. 2021. PMID: 33909660 Free PMC article.
-
The first wave of the SARS-CoV-2 epidemic in Tuscany (Italy): A SI2R2D compartmental model with uncertainty evaluation.PLoS One. 2021 Apr 21;16(4):e0250029. doi: 10.1371/journal.pone.0250029. eCollection 2021. PLoS One. 2021. PMID: 33882085 Free PMC article.
-
Age-Stratified Model to Assess Health Outcomes of COVID-19 Vaccination Strategies, Ghana.Emerg Infect Dis. 2023 Feb;29(2):360-370. doi: 10.3201/eid2902.221098. Epub 2023 Jan 10. Emerg Infect Dis. 2023. PMID: 36626878 Free PMC article.
-
Agent-based epidemiological modeling of COVID-19 in localized environments.Comput Biol Med. 2022 May;144:105396. doi: 10.1016/j.compbiomed.2022.105396. Epub 2022 Mar 11. Comput Biol Med. 2022. PMID: 35299041 Free PMC article.
-
Networks of necessity: Simulating COVID-19 mitigation strategies for disabled people and their caregivers.PLoS Comput Biol. 2022 May 18;18(5):e1010042. doi: 10.1371/journal.pcbi.1010042. eCollection 2022 May. PLoS Comput Biol. 2022. PMID: 35584133 Free PMC article.
References
-
- Russell TW, Hellewell J, Jarvis CI, et al. . Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the diamond Princess cruise SHIP, February 2020. Euro Surveill 2020;25:2000256. 10.2807/1560-7917.ES.2020.25.12.2000256 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous