

The Ethical Dilemma in the Surgical Management of Low Grade Gliomas According to the Variable Availability of Resources and Surgeon Experience
- PMID: 32656117
- PMCID: PMC7335147
- DOI: 10.4103/ajns.AJNS_296_19
The Ethical Dilemma in the Surgical Management of Low Grade Gliomas According to the Variable Availability of Resources and Surgeon Experience
Abstract
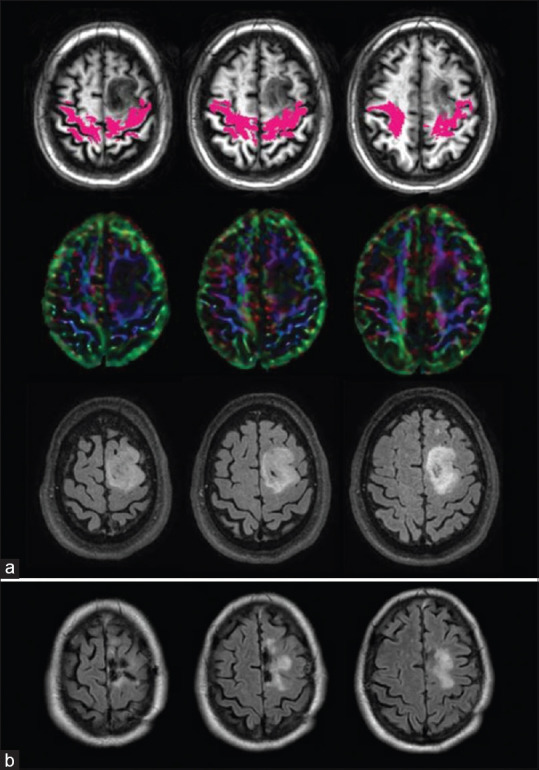
Low grade gliomas (LGGs) affect young individuals in the prime of life. Management may alternatively include biopsy and observation or surgical resection. Recent evidence strongly favors maximal and supramaximal resection of LGGs in optimizing survival metrics. Awake craniotomy with cortical mapping and electrical stimulation along with other preoperative and intraoperative surgical adjuncts, including intraoperative magnetic resonance and diffusion tensor imaging, facilitates maximization of resection and eschews precipitating neurological deficits. Intraoperative imaging permits additional resection of identified residual to be completed within the same surgical session, improving extent of resection and consequently progression free and overall survival. These resources are available in only a few centers throughout the United States, raising an ethical dilemma as to where patients harboring LGGs should most appropriately be treated.
Keywords: Gliomas; intraoperative; magnetic resonance imaging; neuronavigation; supratotal resection; surgeon experience; survival; technology.
Copyright: © 2020 Asian Journal of Neurosurgery.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Awake surgery for WHO Grade II gliomas within "noneloquent" areas in the left dominant hemisphere: toward a "supratotal" resection. Clinical article.J Neurosurg. 2011 Aug;115(2):232-9. doi: 10.3171/2011.3.JNS101333. Epub 2011 May 6. J Neurosurg. 2011. PMID: 21548750
-
Awake Craniotomy with Noninvasive Brain Mapping by 3-Tesla Functional Magnetic Resonance Imaging for Excision of Low-grade Glioma: A Case of a Young Patient from Pakistan.Asian J Neurosurg. 2018 Apr-Jun;13(2):471-474. doi: 10.4103/ajns.AJNS_144_16. Asian J Neurosurg. 2018. PMID: 29682064 Free PMC article.
-
Strategies to maximize resection of complex, or high surgical risk, low-grade gliomas.Neurosurg Focus. 2013 Feb;34(2):E5. doi: 10.3171/2012.12.FOCUS12338. Neurosurg Focus. 2013. PMID: 23373450
-
Supratotal Surgical Resection for Low-Grade Glioma: A Systematic Review.Cancers (Basel). 2023 Apr 26;15(9):2493. doi: 10.3390/cancers15092493. Cancers (Basel). 2023. PMID: 37173957 Free PMC article. Review.
-
Supratotal resection of diffuse gliomas - an overview of its multifaceted implications.Neurochirurgie. 2017 Jun;63(3):243-249. doi: 10.1016/j.neuchi.2016.09.006. Epub 2017 Feb 7. Neurochirurgie. 2017. PMID: 28185647 Review.
References
-
- McKhann GM, Duffau H. Low-grade glioma: Epidemiology, pathophysiology, clinical features, and treatment. Neurosurg Clin N Am. 2019;30:xiii–xiv. - PubMed
-
- Duffau H. Long-term outcomes after supratotal resection of diffuse low-grade gliomas: A consecutive series with 11-year follow-up. Acta Neurochir (Wien) 2016;158:51–8. - PubMed
-
- Duffau H. Awake mapping is not an additional surgical technique but an alternative philosophy in the management of low-grade glioma patients. Neurosurg Rev. 2018;41:689–91. - PubMed