

Genomic Alterations of NTRK, POLE, ERBB2, and Microsatellite Instability Status in Chinese Patients with Colorectal Cancer
- PMID: 32627883
- PMCID: PMC7648350
- DOI: 10.1634/theoncologist.2020-0356
Genomic Alterations of NTRK, POLE, ERBB2, and Microsatellite Instability Status in Chinese Patients with Colorectal Cancer
Abstract
Background: The increasing molecular characterization of colorectal cancers (CRCs) has spurred the need to look beyond RAS, BRAF, and microsatellite instability (MSI). Genomic alterations, including ERBB2 amplifications and mutations, POLE mutations, MSI, and NTRK1-3 fusions, have emerged as targets for matched therapies. We sought to study a clinically annotated Chinese cohort of CRC subjected to genomic profiling to explore relative target frequencies.
Methods: Tumor and matched whole blood were collected from 609 Chinese patients with CRC. Extracted DNA was analyzed for all classes of genomic alterations across 450 cancer-related genes, including single-nucleotide variations (SNVs), short and long insertions and deletions (indels), copy number variations, and gene rearrangements. Next-generation sequencing-based computational algorithms also determined tumor mutational burden and MSI status.
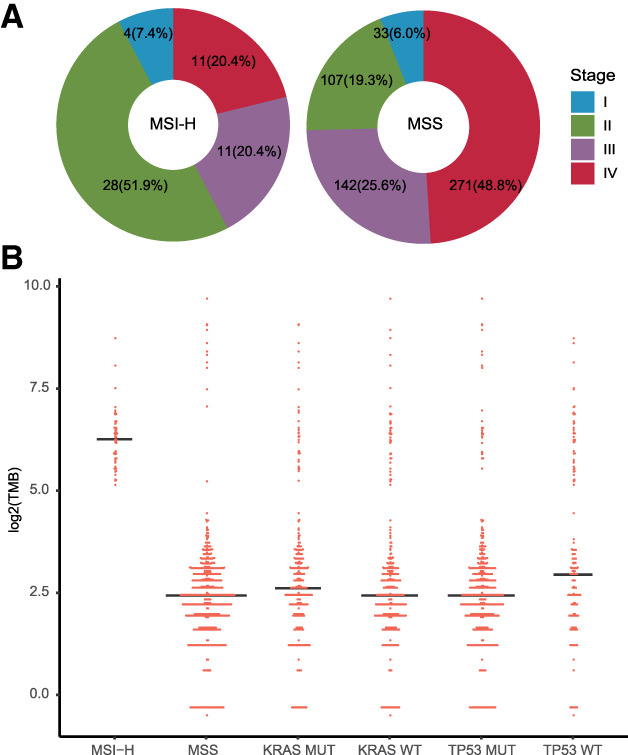
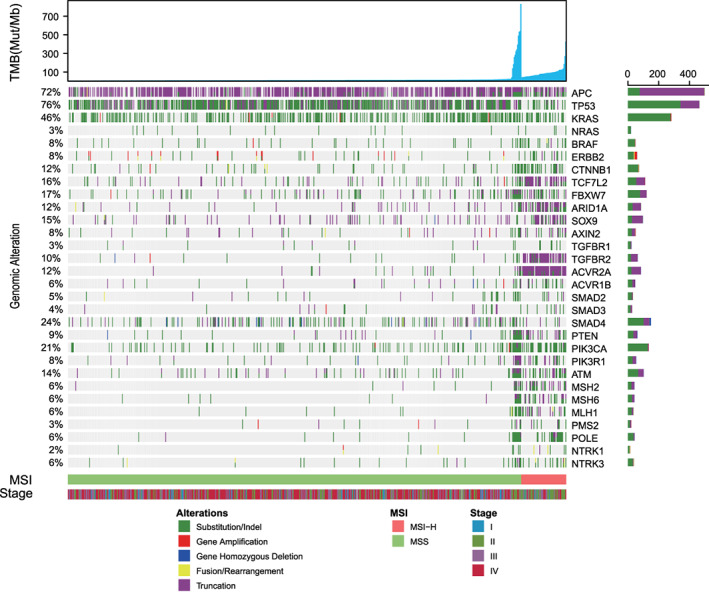
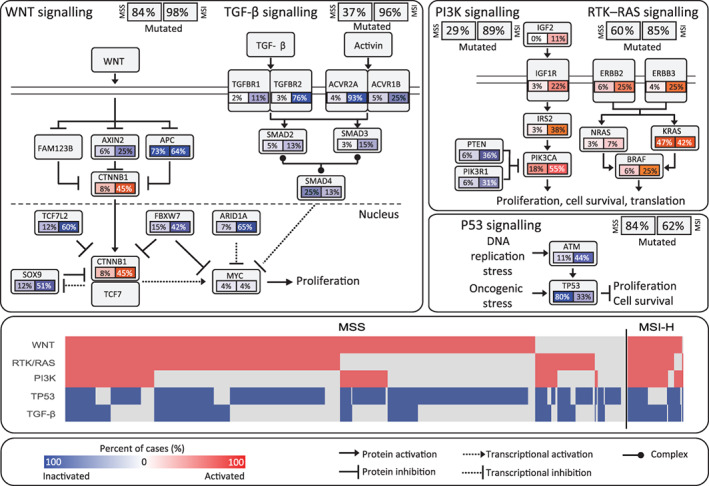
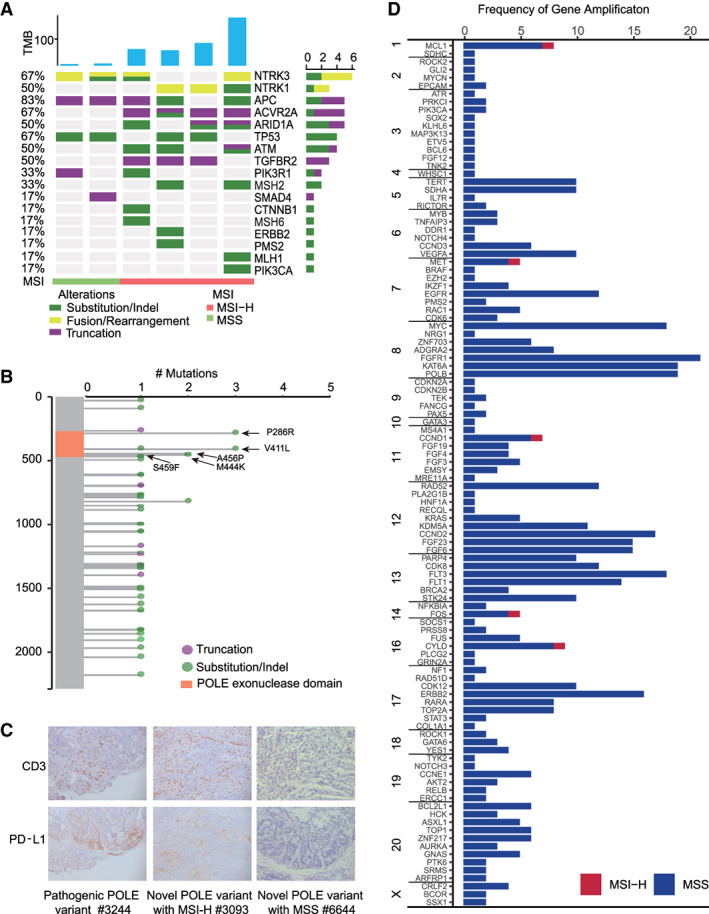
Results: Alterations in TP53 (76%), APC (72%), and KRAS (46%) were common in Chinese patients with CRC. For the first time, the prevalence of NTRK gene fusion was observed to be around 7% in the MSI-high CRC cohort. Across the cohort, MSI was found in 9%, ERBB2 amplification in 3%, and POLE pathogenic mutation in 1.5% of patients. Such results mostly parallel frequencies observed in Western patients. However, POLE existed at a higher frequency and was associated with large tumor T-cell infiltration.
Conclusion: Comparing to the Western counterparts, POLE mutations were increased in our cohort. The prevalence of NTRK gene fusion was around 7% in the MSI-high CRC cohort. Increased adoption of molecular profiling in Asian patients is essential for the improvement of therapeutic outcomes.
Implications for practice: The increasing use of genomic profiling assays in colorectal cancer (CRC) has allowed for the identification of a higher number of patient subsets benefiting from matched therapies. With an increase in the number of therapies, assays simultaneously evaluating all candidate biomarkers are critical. The results of this study provide an early support for the feasibility and utility of genomic profiling in Chinese patients with CRC.
Keywords: Colorectal cancer; DNA polymerase ε; ERBB2 amplification; Tropomyosin receptor kinase; Tumor mutational burden.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
Similar articles
-
Genomic profiling of colorectal cancer in large-scale Chinese patients: amplification and somatic mutations in ERBB2.Oncol Res. 2024 Aug 23;32(9):1429-1438. doi: 10.32604/or.2024.047309. eCollection 2024. Oncol Res. 2024. PMID: 39220126 Free PMC article.
-
Genomic Alterations and Clinical Characterization in Chinese Patients with Metastatic Colorectal Cancer.Discov Med. 2024 Jul;36(186):1477-1485. doi: 10.24976/Discov.Med.202436186.137. Discov Med. 2024. PMID: 39054718
-
A comprehensive analysis of POLE/POLD1 genomic alterations in colorectal cancer.Oncologist. 2024 Sep 6;29(9):e1224-e1227. doi: 10.1093/oncolo/oyae098. Oncologist. 2024. PMID: 38776551 Free PMC article.
-
Molecular Profiling in Metastatic Colorectal Cancer.Oncology (Williston Park). 2020 Sep 15;34(9):352-355. doi: 10.46883/ONC.2020.3409.0352. Oncology (Williston Park). 2020. PMID: 32965665 Review.
-
Incorporating traditional and emerging biomarkers in the clinical management of metastatic colorectal cancer: an update.Expert Rev Mol Diagn. 2020 Jul;20(7):653-664. doi: 10.1080/14737159.2020.1782194. Epub 2020 Jun 22. Expert Rev Mol Diagn. 2020. PMID: 32552041 Review.
Cited by
-
Gene fusions and oncogenic mutations in MLH1 deficient and BRAFV600E wild-type colorectal cancers.Virchows Arch. 2022 Apr;480(4):807-817. doi: 10.1007/s00428-022-03302-x. Epub 2022 Mar 3. Virchows Arch. 2022. PMID: 35237889 Free PMC article.
-
RAS/RAF mutations and microsatellite instability status in primary colorectal cancers according to HER2 amplification.Sci Rep. 2024 May 19;14(1):11432. doi: 10.1038/s41598-024-62096-x. Sci Rep. 2024. PMID: 38763942 Free PMC article.
-
NTRK fusion in Japanese colorectal adenocarcinomas.Sci Rep. 2021 Mar 11;11(1):5635. doi: 10.1038/s41598-021-85075-y. Sci Rep. 2021. PMID: 33707574 Free PMC article.
-
Prevalence and clinico-genomic characteristics of patients with TRK fusion cancer in China.NPJ Precis Oncol. 2023 Aug 11;7(1):75. doi: 10.1038/s41698-023-00427-3. NPJ Precis Oncol. 2023. PMID: 37567953 Free PMC article.
-
NTRK fusion positive colorectal cancer is a unique subset of CRC with high TMB and microsatellite instability.Cancer Med. 2022 Jul;11(13):2541-2549. doi: 10.1002/cam4.4561. Epub 2022 May 4. Cancer Med. 2022. PMID: 35506567 Free PMC article.
References
-
- Chen W, Zheng R, Baade PD et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115–132. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
