

Treatment of MOG antibody associated disorders: results of an international survey
- PMID: 32623595
- PMCID: PMC7954658
- DOI: 10.1007/s00415-020-10026-y
Treatment of MOG antibody associated disorders: results of an international survey
Abstract
Introduction: While monophasic and relapsing forms of myelin oligodendrocyte glycoprotein antibody associated disorders (MOGAD) are increasingly diagnosed world-wide, consensus on management is yet to be developed.
Objective: To survey the current global clinical practice of clinicians treating MOGAD.
Method: Neurologists worldwide with expertise in treating MOGAD participated in an online survey (February-April 2019).
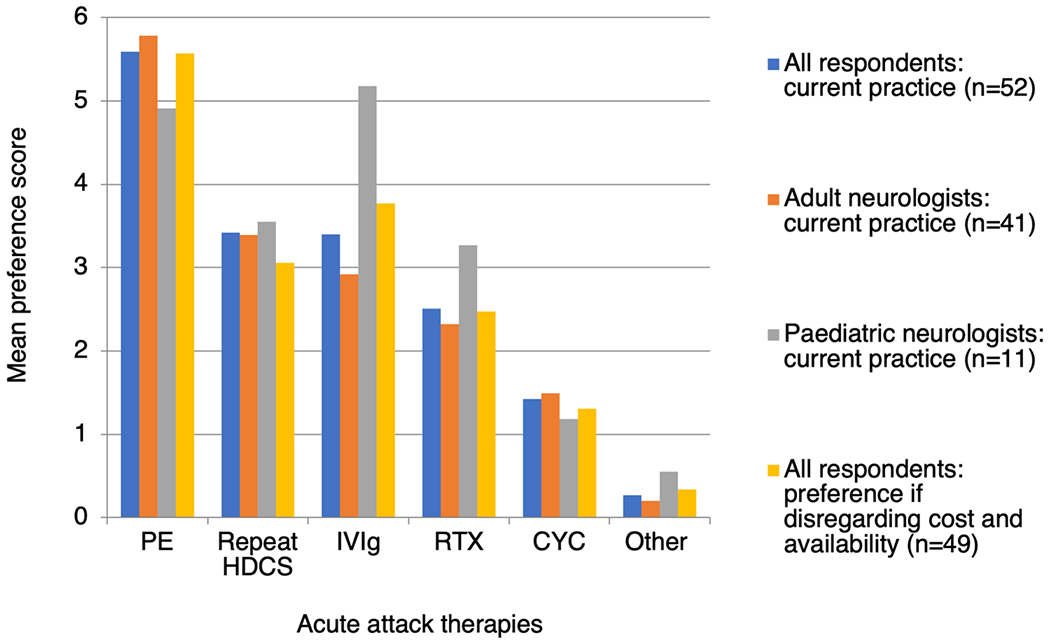
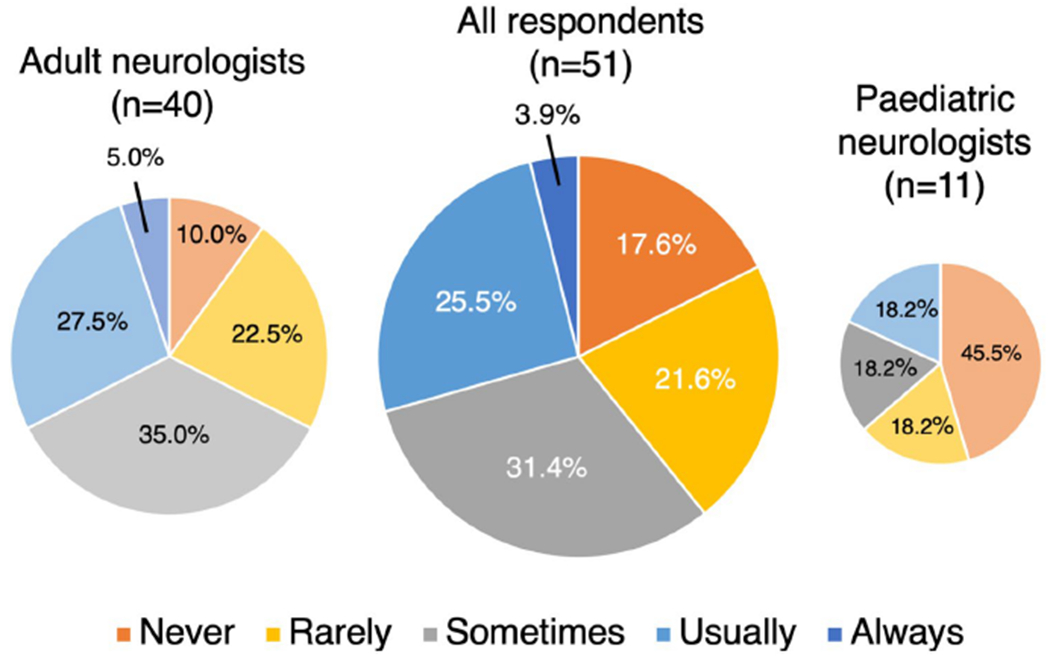
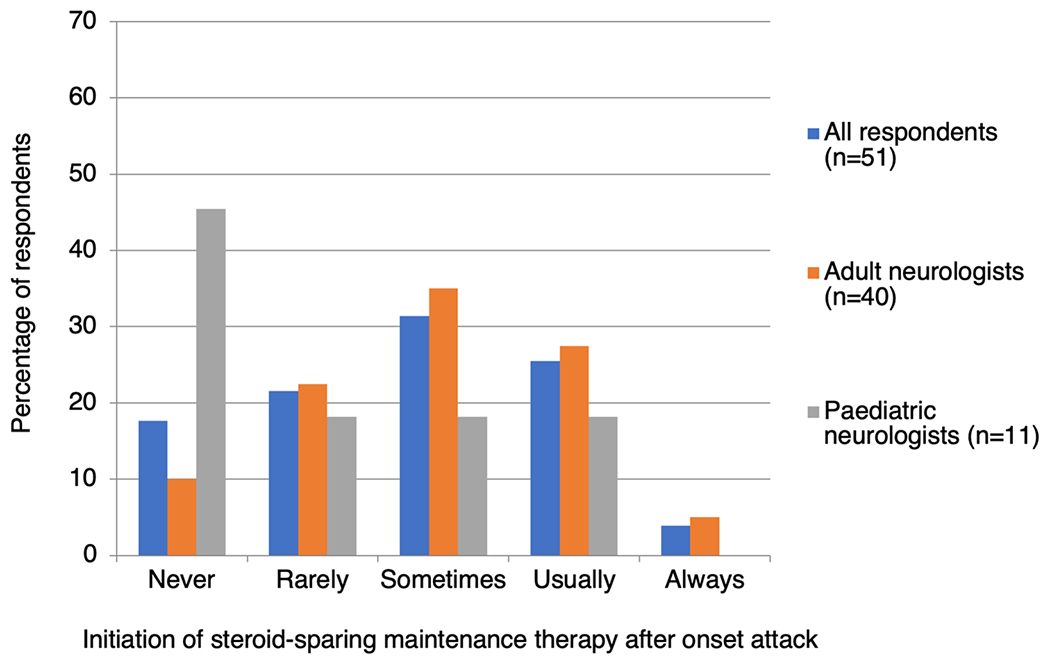
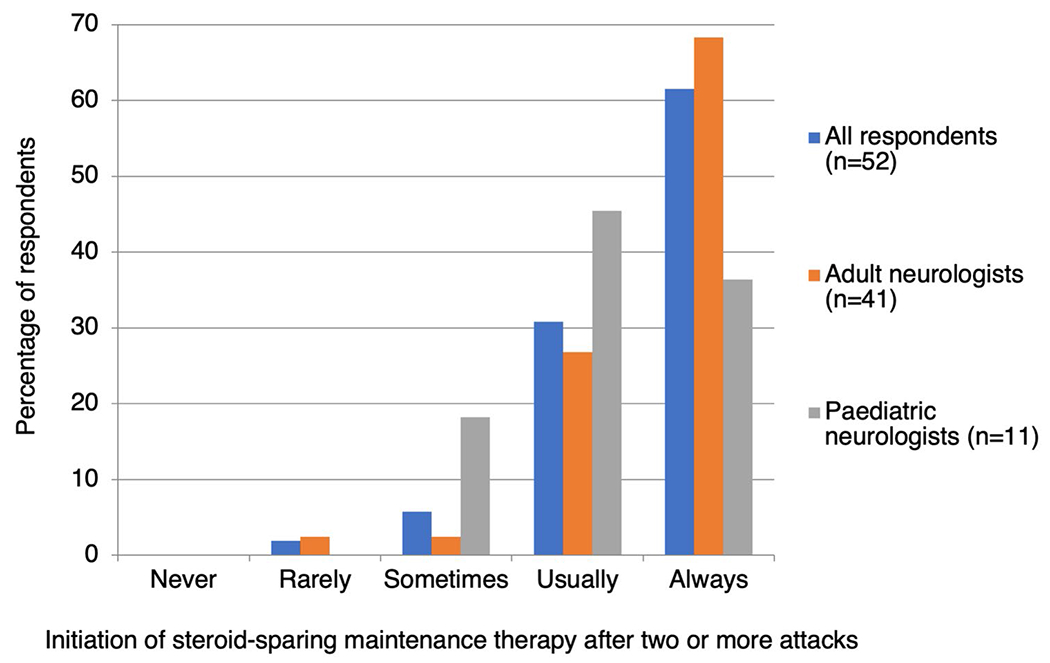
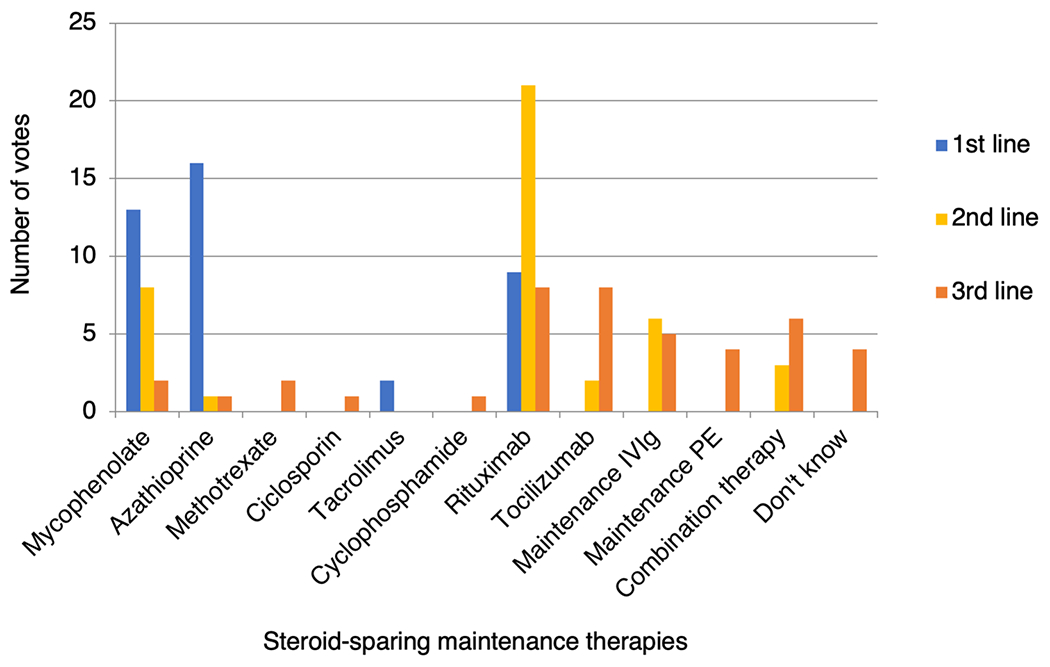
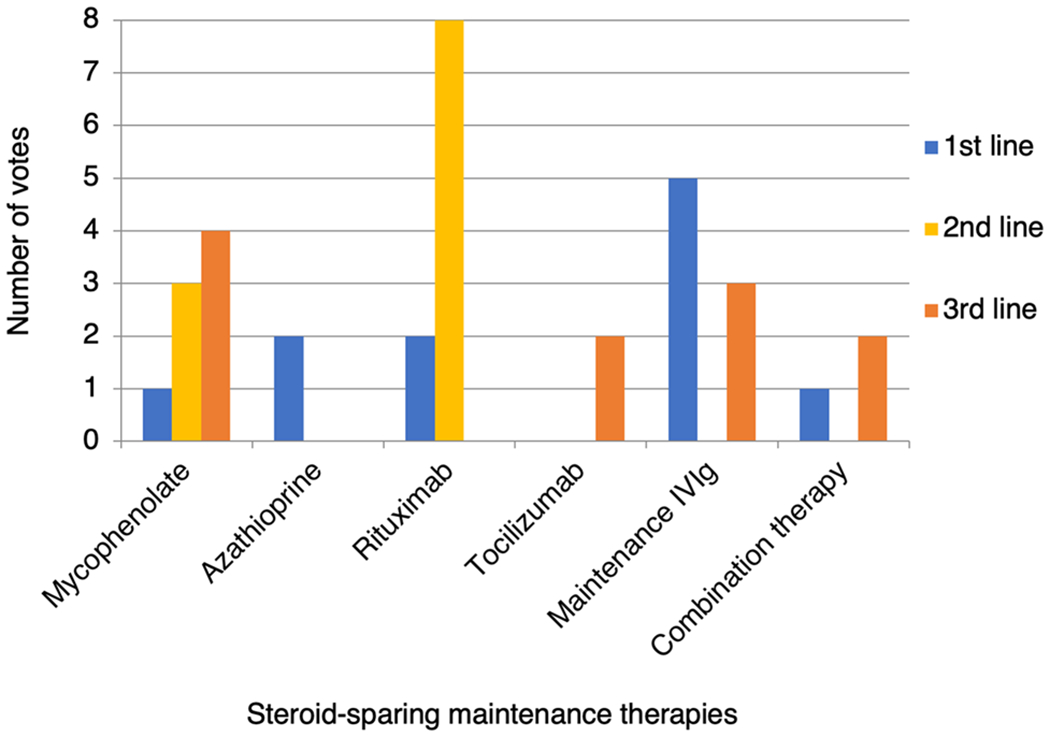
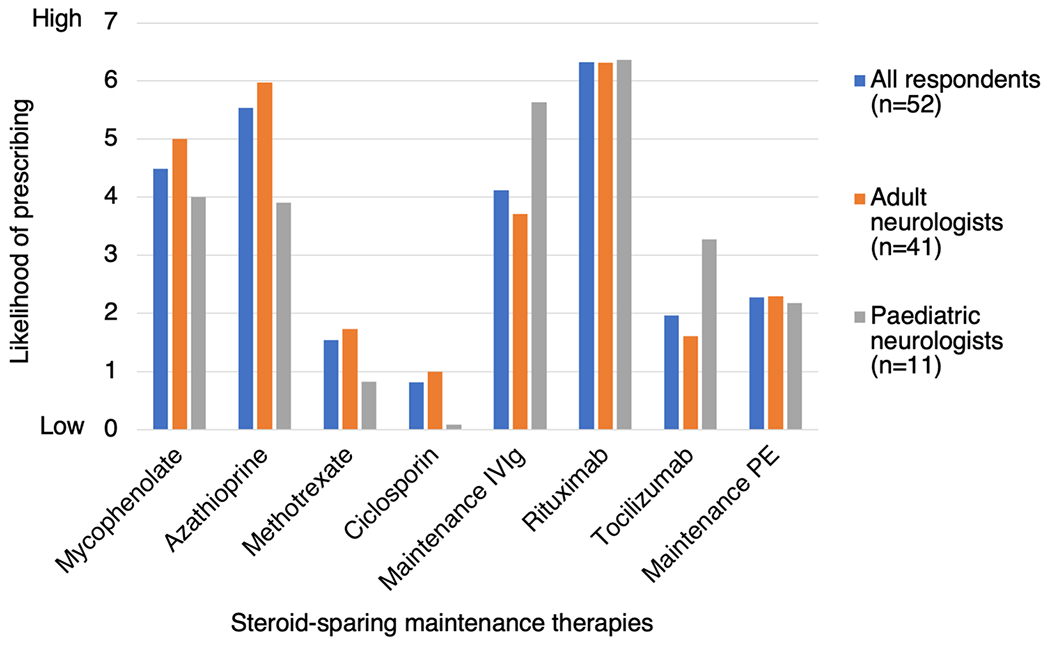
Results: Fifty-two responses were received (response rate 60.5%) from 86 invited experts, comprising adult (78.8%, 41/52) and paediatric (21.2%, 11/52) neurologists in 22 countries. All treat acute attacks with high dose corticosteroids. If recovery is incomplete, 71.2% (37/52) proceed next to plasma exchange (PE). 45.5% (5/11) of paediatric neurologists use IV immunoglobulin (IVIg) in preference to PE. Following an acute attack, 55.8% (29/52) of respondents typically continue corticosteroids for ≥ 3 months; though less commonly when treating children. After an index event, 60% (31/51) usually start steroid-sparing maintenance therapy (MT); after ≥ 2 attacks 92.3% (48/52) would start MT. Repeat MOG antibody status is used by 52.9% (27/51) to help decide on MT initiation. Commonly used first line MTs in adults are azathioprine (30.8%, 16/52), mycophenolate mofetil (25.0%, 13/52) and rituximab (17.3%, 9/52). In children, IVIg is the preferred first line MT (54.5%; 6/11). Treatment response is monitored by MRI (53.8%; 28/52), optical coherence tomography (23.1%; 12/52) and MOG antibody titres (36.5%; 19/52). Regardless of monitoring results, 25.0% (13/52) would not stop MT.
Conclusion: Current treatment of MOGAD is highly variable, indicating a need for consensus-based treatment guidelines, while awaiting definitive clinical trials.
Keywords: MOG; MOGAD; Myelin oligodendrocyte glycoprotein; Survey.
Figures
Similar articles
-
E.U. paediatric MOG consortium consensus: Part 5 - Treatment of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders.Eur J Paediatr Neurol. 2020 Nov;29:41-53. doi: 10.1016/j.ejpn.2020.10.005. Epub 2020 Nov 4. Eur J Paediatr Neurol. 2020. PMID: 33176999 Review.
-
Treatment of MOG-IgG associated disease in paediatric patients: A systematic review.Mult Scler Relat Disord. 2021 Nov;56:103216. doi: 10.1016/j.msard.2021.103216. Epub 2021 Aug 15. Mult Scler Relat Disord. 2021. PMID: 34450460 Review.
-
Association of Maintenance Intravenous Immunoglobulin With Prevention of Relapse in Adult Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease.JAMA Neurol. 2022 May 1;79(5):518-525. doi: 10.1001/jamaneurol.2022.0489. JAMA Neurol. 2022. PMID: 35377395 Free PMC article.
-
Pediatric myelin oligodendrocyte glycoprotein antibody-associated disease in southern China: analysis of 93 cases.Front Immunol. 2023 Jun 2;14:1162647. doi: 10.3389/fimmu.2023.1162647. eCollection 2023. Front Immunol. 2023. PMID: 37342342 Free PMC article.
-
Myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease: Presentation and outcomes of adults at a single center.J Neuroimmunol. 2022 Dec 15;373:577987. doi: 10.1016/j.jneuroim.2022.577987. Epub 2022 Oct 14. J Neuroimmunol. 2022. PMID: 36272183
Cited by
-
Anti-myelin oligodendrocyte glycoprotein antibodies in a girl with good recovery after five episodes of prior idiopathic optic neuritis.Am J Ophthalmol Case Rep. 2021 Mar 24;22:101060. doi: 10.1016/j.ajoc.2021.101060. eCollection 2021 Jun. Am J Ophthalmol Case Rep. 2021. PMID: 33997466 Free PMC article.
-
Rare Encephalitis-Like Presentation of a Pediatric Patient with Dual Positive Aquaporin-4 and Myelin Oligodendrocyte Antibodies: A Case Report with Review of Literature.Ann Indian Acad Neurol. 2023 Nov-Dec;26(6):1021-1024. doi: 10.4103/aian.aian_689_23. Epub 2023 Oct 31. Ann Indian Acad Neurol. 2023. PMID: 38229648 Free PMC article. No abstract available.
-
Long-term Effectiveness and Safety of Rituximab in Neuromyelitis Optica Spectrum Disorder and MOG Antibody Disease.Neurology. 2022 Nov 29;99(22):e2504-e2516. doi: 10.1212/WNL.0000000000201260. Epub 2022 Aug 31. Neurology. 2022. PMID: 36240094 Free PMC article.
-
Extensive brainstem lesions in myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): A case report.Radiol Case Rep. 2024 Sep 6;19(12):5589-5594. doi: 10.1016/j.radcr.2024.08.032. eCollection 2024 Dec. Radiol Case Rep. 2024. PMID: 39296754 Free PMC article.
-
Relapsing MRI-negative myelitis associated with myelin-oligodendrocyte glycoprotein autoantibodies: a case report.BMC Neurol. 2022 Aug 24;22(1):313. doi: 10.1186/s12883-022-02837-5. BMC Neurol. 2022. PMID: 36002821 Free PMC article.
References
-
- Jarius S, Ruprecht K, Kleiter I et al. (2016) MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 2: Epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome. J Neuroinflamm 13(1):280. 10.1186/s12974-016-0718-0 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
