

COVID-19 Pandemic: Cardiovascular Complications and Future Implications
- PMID: 32578167
- PMCID: PMC7310596
- DOI: 10.1007/s40256-020-00420-2
COVID-19 Pandemic: Cardiovascular Complications and Future Implications
Abstract
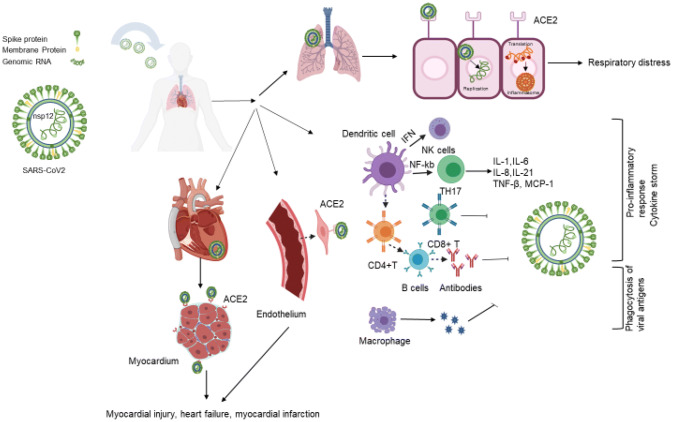
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is now a global pandemic with the highest number of affected individuals in the modern era. Not only is the infection inflicting significant morbidity and mortality, but there has also been a significant strain to the health care system and the economy. COVID-19 typically presents as viral pneumonia, occasionally leading to acute respiratory distress syndrome (ARDS) and death. However, emerging evidence suggests that it has a significant impact on the cardiovascular (CV) system by direct myocardial damage, severe systemic inflammatory response, hypoxia, right heart strain secondary to ARDS and lung injury, and plaque rupture secondary to inflammation. Primary cardiac manifestations include acute myocarditis, myocardial infarction, arrhythmia, and abnormal clotting. Several consensus documents have been released to help manage CV disease during this pandemic. In this review, we summarize key cardiac manifestations, their management, and future implications.
Conflict of interest statement
Dr. Gregg C. Fonarow reports research funding from the NIH and serving as a consultant for Abbott, Amgen, AstraZeneca, Bayer, CHF Solutions, Janssen, Medtronic, Merck, and Novartis. Dhrubajyoti Bandyopadhyay, Tauseef Akhtar, Adrija Hajra, Manasvi Gupta, Avash Das, Sandipan Chakraborty, Ipsita Pal, Neelkumar Patel, Birendra Amgai, Raktim K. Ghosh, Carl J. Lavie, and Srihari S. Naidu declare they have no potential conflicts of interest that might be relevant to the contents of this article.
Figures
Similar articles
-
COVID-19 pandemic and cardiovascular disease: where do we stand?Minerva Cardioangiol. 2020 Aug;68(4):347-358. doi: 10.23736/S0026-4725.20.05298-6. Epub 2020 May 29. Minerva Cardioangiol. 2020. PMID: 32472990 Review.
-
Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome.Circulation. 2020 Jun 9;141(23):1903-1914. doi: 10.1161/CIRCULATIONAHA.120.047349. Epub 2020 Apr 16. Circulation. 2020. PMID: 32297796 Free PMC article. Review.
-
Pathogenic mechanisms of cardiovascular damage in COVID-19.Mol Med. 2024 Jun 19;30(1):92. doi: 10.1186/s10020-024-00855-2. Mol Med. 2024. PMID: 38898389 Free PMC article. Review.
-
Myocardial injury and COVID-19: Possible mechanisms.Life Sci. 2020 Jul 15;253:117723. doi: 10.1016/j.lfs.2020.117723. Epub 2020 Apr 28. Life Sci. 2020. PMID: 32360126 Free PMC article. Review.
-
COVID-19 and the Cardiovascular System.Crit Care Nurs Q. 2020 Oct/Dec;43(4):381-389. doi: 10.1097/CNQ.0000000000000323. Crit Care Nurs Q. 2020. PMID: 32833774 Review.
Cited by
-
SARS2 simplified scores to estimate risk of hospitalization and death among patients with COVID-19.medRxiv [Preprint]. 2020 Sep 13:2020.09.11.20190520. doi: 10.1101/2020.09.11.20190520. medRxiv. 2020. Update in: Sci Rep. 2021 Mar 2;11(1):4945. doi: 10.1038/s41598-021-84603-0 PMID: 32935112 Free PMC article. Updated. Preprint.
-
The Correlation between Cardiac Magnetic Resonance Findings and Post-COVID-19: The Impact of Myocardial Injury on Quality of Life.Diagnostics (Basel). 2024 Sep 2;14(17):1937. doi: 10.3390/diagnostics14171937. Diagnostics (Basel). 2024. PMID: 39272722 Free PMC article.
-
Clinical and angiographic characteristics of patients with STEMI and confirmed diagnosis of COVID-19: an experience of Tanta University Hospital.Egypt Heart J. 2020 Oct 6;72(1):68. doi: 10.1186/s43044-020-00103-y. Egypt Heart J. 2020. PMID: 33025310 Free PMC article.
-
Potential long-term effects of SARS-CoV-2 infection on the pulmonary vasculature: Multilayered cross-talks in the setting of coinfections and comorbidities.PLoS Pathog. 2023 Jan 12;19(1):e1011063. doi: 10.1371/journal.ppat.1011063. eCollection 2023 Jan. PLoS Pathog. 2023. PMID: 36634048 Free PMC article. Review.
-
SARS2 simplified scores to estimate risk of hospitalization and death among patients with COVID-19.Sci Rep. 2021 Mar 2;11(1):4945. doi: 10.1038/s41598-021-84603-0. Sci Rep. 2021. PMID: 33654180 Free PMC article.
References
-
- Callaway E, Cyranoski D, Mallapaty S, Stoye E, Tollefson J. The coronavirus pandemic in five powerful charts. Nature. 2020;579(7800):482–483. - PubMed
-
- Centers for Disease Control and Prevention. Cases in the US. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html.... Accessed 29 May 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
