

MSC Therapies for COVID-19: Importance of Patient Coagulopathy, Thromboprophylaxis, Cell Product Quality and Mode of Delivery for Treatment Safety and Efficacy
- PMID: 32574263
- PMCID: PMC7249852
- DOI: 10.3389/fimmu.2020.01091
MSC Therapies for COVID-19: Importance of Patient Coagulopathy, Thromboprophylaxis, Cell Product Quality and Mode of Delivery for Treatment Safety and Efficacy
Abstract
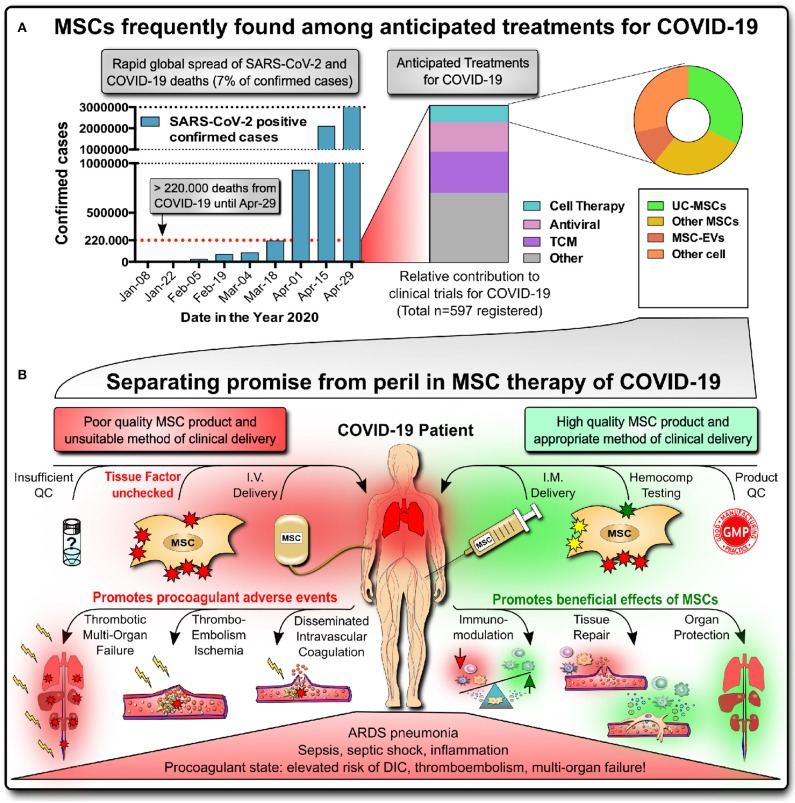
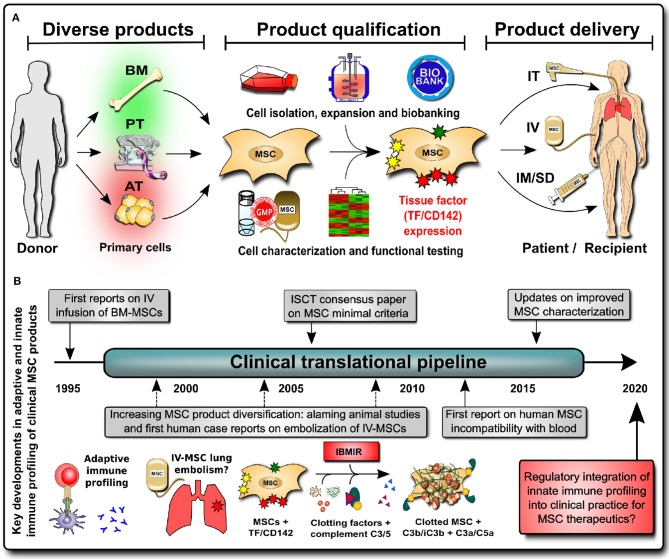
Numerous clinical trials of mesenchymal stromal/stem cells (MSCs) as a new treatment for coronavirus-induced disease (COVID-19) have been registered recently, most of them based on intravenous (IV) infusion. There is no approved effective therapy for COVID-19, but MSC therapies have shown first promise in the treatment of acute respiratory distress syndrome (ARDS) pneumonia, inflammation, and sepsis, which are among the leading causes of mortality in COVID-19 patients. Many of the critically ill COVID-19 patients are in a hypercoagulable procoagulant state and at high risk for disseminated intravascular coagulation, thromboembolism, and thrombotic multi-organ failure, another cause of high fatality. It is not yet clear whether IV infusion is a safe and effective route of MSC delivery in COVID-19, since MSC-based products express variable levels of highly procoagulant tissue factor (TF/CD142), compromising the cells' hemocompatibility and safety profile. Of concern, IV infusions of poorly characterized MSC products with unchecked (high) TF/CD142 expression could trigger blood clotting in COVID-19 and other vulnerable patient populations and further promote the risk for thromboembolism. In contrast, well-characterized products with robust manufacturing procedures and optimized modes of clinical delivery hold great promise for ameliorating COVID-19 by exerting their beneficial immunomodulatory effects, inducing tissue repair and organ protection. While the need for MSC therapy in COVID-19 is apparent, integrating both innate and adaptive immune compatibility testing into the current guidelines for cell, tissue, and organ transplantation is critical for safe and effective therapies. It is paramount to only use well-characterized, safe MSCs even in the most urgent and experimental treatments. We here propose three steps to mitigate the risk for these vulnerable patients: (1) updated clinical guidelines for cell and tissue transplantation, (2) updated minimal criteria for characterization of cellular therapeutics, and (3) updated cell therapy routines reflecting specific patient needs.
Keywords: coagulation/clotting/thrombosis; coronavirus-induced disease 2019 (COVID19); hemocompatibility testing; intensive care unit (ICU); intravascular and intravenous infusion; mesenchymal stromal cells (MSC); severe acute respiratory distress syndrome coronavirus-2 (SARS-CoV-2); tissue factor (TF/CD142).
Copyright © 2020 Moll, Drzeniek, Kamhieh-Milz, Geissler, Volk and Reinke.
Figures
Similar articles
-
Potential application of mesenchymal stem cells and their exosomes in lung injury: an emerging therapeutic option for COVID-19 patients.Stem Cell Res Ther. 2020 Oct 15;11(1):437. doi: 10.1186/s13287-020-01963-6. Stem Cell Res Ther. 2020. PMID: 33059757 Free PMC article. Review.
-
Safety and Effectiveness of Intravascular Mesenchymal Stem Cells to Treat Organ Failure and Possible Application in COVID-19 Complications.Pain Physician. 2020 Aug;23(4S):S391-S420. Pain Physician. 2020. PMID: 32942796 Review.
-
Improved MSC Minimal Criteria to Maximize Patient Safety: A Call to Embrace Tissue Factor and Hemocompatibility Assessment of MSC Products.Stem Cells Transl Med. 2022 Mar 3;11(1):2-13. doi: 10.1093/stcltm/szab005. Stem Cells Transl Med. 2022. PMID: 35641163 Free PMC article.
-
Rationale for the clinical use of adipose-derived mesenchymal stem cells for COVID-19 patients.J Transl Med. 2020 May 18;18(1):203. doi: 10.1186/s12967-020-02380-2. J Transl Med. 2020. PMID: 32423449 Free PMC article. Review.
-
Expanded Umbilical Cord Mesenchymal Stem Cells (UC-MSCs) as a Therapeutic Strategy in Managing Critically Ill COVID-19 Patients: The Case for Compassionate Use.Pain Physician. 2020 Mar;23(2):E71-E83. Pain Physician. 2020. PMID: 32214286
Cited by
-
Advanced cell therapy with low tissue factor loaded product NestaCell® does not confer thrombogenic risk for critically ill COVID-19 heparin-treated patients.Biomed Pharmacother. 2022 May;149:112920. doi: 10.1016/j.biopha.2022.112920. Epub 2022 Apr 1. Biomed Pharmacother. 2022. PMID: 36068779 Free PMC article.
-
Mesenchymal Stem Cells and Their Extracellular Vesicles: A Potential Game Changer for the COVID-19 Crisis.Front Cell Dev Biol. 2020 Sep 30;8:587866. doi: 10.3389/fcell.2020.587866. eCollection 2020. Front Cell Dev Biol. 2020. PMID: 33102489 Free PMC article.
-
The Epidermal Keratinocyte as a Therapeutic Target for Management of Diabetic Wounds.Int J Mol Sci. 2023 Feb 21;24(5):4290. doi: 10.3390/ijms24054290. Int J Mol Sci. 2023. PMID: 36901720 Free PMC article. Review.
-
Are We Ready for Cell Therapy to Treat Stroke?Front Cell Dev Biol. 2021 Jun 23;9:621645. doi: 10.3389/fcell.2021.621645. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34249901 Free PMC article. Review.
-
Emerging therapeutics in the management of COVID-19.World J Virol. 2021 Jan 25;10(1):1-29. doi: 10.5501/wjv.v10.i1.1. World J Virol. 2021. PMID: 33585175 Free PMC article. Review.
References
-
- Nacoti M, Ciocca A, Giupponi A, Brambillasca P, Lussana F, Pisano M, et al. At the epicenter of the Covid-19 pandemic and humanitarian crises in Italy: changing perspectives on preparation and mitigation. Catalyst Non Issue Content. (2020) 1 10.1186/s12939-020-01162-y - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous