

Towards new horizons: characterization, classification and implications of the tumour antigenic repertoire
- PMID: 32572208
- PMCID: PMC7306938
- DOI: 10.1038/s41571-020-0387-x
Towards new horizons: characterization, classification and implications of the tumour antigenic repertoire
Abstract
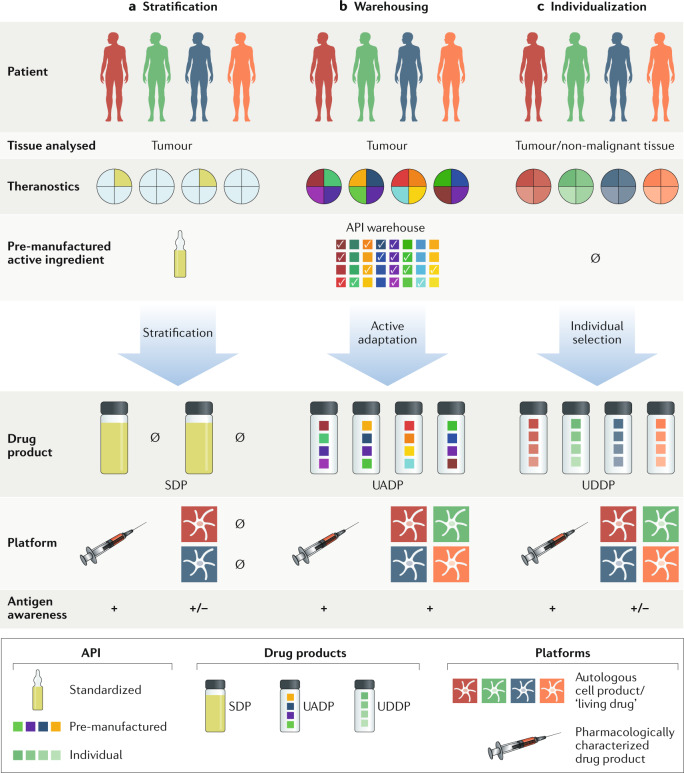
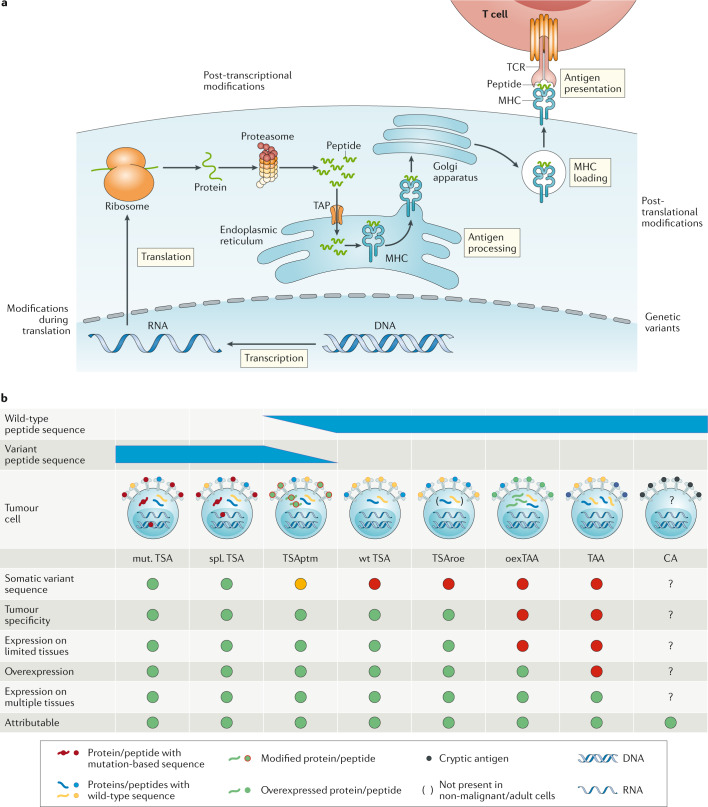
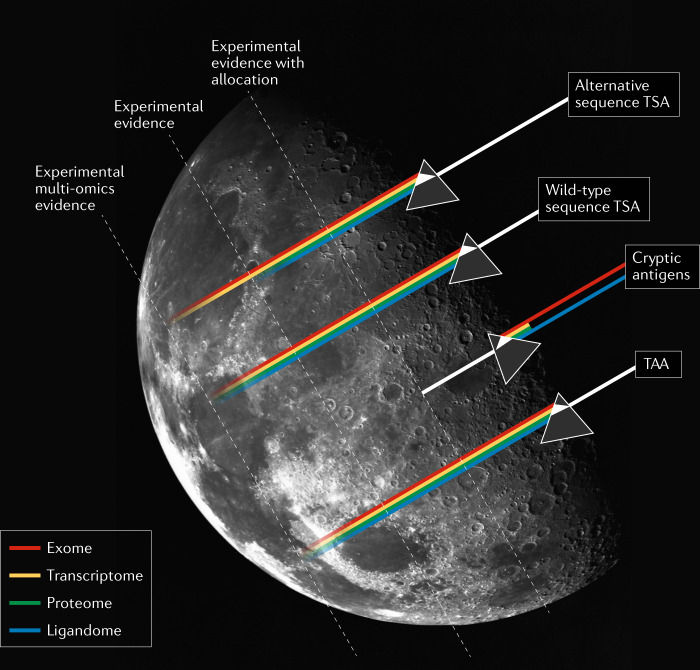
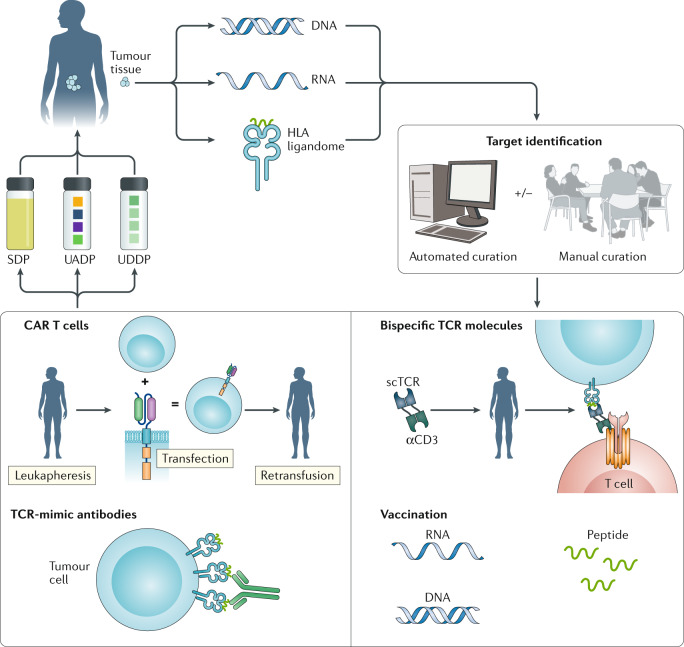
Immune-checkpoint inhibition provides an unmatched level of durable clinical efficacy in various malignancies. Such therapies promote the activation of antigen-specific T cells, although the precise targets of these T cells remain unknown. Exploiting these targets holds great potential to amplify responses to treatment, such as by combining immune-checkpoint inhibition with therapeutic vaccination or other antigen-directed treatments. In this scenario, the pivotal hurdle remains the definition of valid HLA-restricted tumour antigens, which requires several levels of evidence before targets can be established with sufficient confidence. Suitable antigens might include tumour-specific antigens with alternative or wild-type sequences, tumour-associated antigens and cryptic antigens that exceed exome boundaries. Comprehensive antigen classification is required to enable future clinical development and the definition of innovative treatment strategies. Furthermore, clinical development remains challenging with regard to drug manufacturing and regulation, as well as treatment feasibility. Despite these challenges, treatments based on diligently curated antigens combined with a suitable therapeutic platform have the potential to enable optimal antitumour efficacy in patients, either as monotherapies or in combination with other established immunotherapies. In this Review, we summarize the current state-of-the-art approaches for the identification of candidate tumour antigens and provide a structured terminology based on their underlying characteristics.
Conflict of interest statement
S.P.H. has acted as an advisory board member for Abbvie, Bristol–Myers Squibb, MSD and Roche, and is a co-inventor of several patents owned by Immatics Biotechnologies. M.W.L. is a co-inventor of several patents owned by Immatics Biotechnologies, and has acted as a consultant and/or advisory board member for Boehringer Ingelheim. H.-G.R. has ownership interest (including shares) in CureVac, Immatics Biotechnologies and Synimmune, is a co-inventor and/or has shared interests in several patents held by CureVac, Immatics Biotechnologies and Synimmune, and is a co-inventor and shares the patent for the adjuvant candidate XS15. P.B. has acted as a consultant or advisory board member for Amgen, AstraZeneca, Bristol–Myers Squibb, MSD and Roche, has received speaker’s fees from Abbvie, AstraZeneca, Bristol-Myers Squibb, and MSD, and has ownership interests in Immatics Biotechnologies.
Figures
Similar articles
-
Genetically modified tumour vaccines--where we are today.Cancer Treat Rev. 1999 Feb;25(1):29-46. doi: 10.1053/ctrv.1998.0104. Cancer Treat Rev. 1999. PMID: 10212588 Review.
-
Human antigen-presenting cell/tumour cell hybrids stimulate strong allogeneic responses and present tumour-associated antigens to cytotoxic T cells in vitro.Immunology. 1999 Dec;98(4):541-50. doi: 10.1046/j.1365-2567.1999.00912.x. Immunology. 1999. PMID: 10594686 Free PMC article.
-
Turning tumour cells into antigen presenting cells: The next step to improve cancer immunotherapy?Eur J Cancer. 2016 Nov;68:134-147. doi: 10.1016/j.ejca.2016.09.010. Epub 2016 Oct 15. Eur J Cancer. 2016. PMID: 27755997 Review.
-
Finding the Keys to the CAR: Identifying Novel Target Antigens for T Cell Redirection Immunotherapies.Int J Mol Sci. 2020 Jan 14;21(2):515. doi: 10.3390/ijms21020515. Int J Mol Sci. 2020. PMID: 31947597 Free PMC article. Review.
-
Glioma antigen.Adv Exp Med Biol. 2012;746:77-84. doi: 10.1007/978-1-4614-3146-6_6. Adv Exp Med Biol. 2012. PMID: 22639160 Review.
Cited by
-
Beneficial autoimmunity improves cancer prognosis.Nat Rev Clin Oncol. 2021 Sep;18(9):591-602. doi: 10.1038/s41571-021-00508-x. Epub 2021 May 11. Nat Rev Clin Oncol. 2021. PMID: 33976418 Review.
-
Relevance of mutation-derived neoantigens and non-classical antigens for anticancer therapies.Hum Vaccin Immunother. 2024 Dec 31;20(1):2303799. doi: 10.1080/21645515.2024.2303799. Epub 2024 Feb 12. Hum Vaccin Immunother. 2024. PMID: 38346926 Free PMC article. Review.
-
Exhaust the exhausters: Targeting regulatory T cells in the tumor microenvironment.Front Immunol. 2022 Sep 30;13:940052. doi: 10.3389/fimmu.2022.940052. eCollection 2022. Front Immunol. 2022. PMID: 36248808 Free PMC article. Review.
-
The Importance of Being Presented: Target Validation by Immunopeptidomics for Epitope-Specific Immunotherapies.Front Immunol. 2022 Apr 6;13:883989. doi: 10.3389/fimmu.2022.883989. eCollection 2022. Front Immunol. 2022. PMID: 35464395 Free PMC article. Review.
-
Incorporation of Toll-Like Receptor Ligands and Inflammasome Stimuli in GM3 Liposomes to Induce Dendritic Cell Maturation and T Cell Responses.Front Immunol. 2022 Feb 18;13:842241. doi: 10.3389/fimmu.2022.842241. eCollection 2022. Front Immunol. 2022. PMID: 35251040 Free PMC article.
References
-
- Schwartz RS. Paul Ehrlich’s magic bullets. N. Engl. J. Med. 2004;350:1079–1080. - PubMed
-
- Thomas ED, Lochte HL, Jr., Lu WC, Ferrebee JW. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957;257:491–496. - PubMed
-
- Kolb HJ, et al. Donor leukocyte transfusions for treatment of recurrent chronic myelogenous leukemia in marrow transplant patients. Blood. 1990;76:2462–2465. - PubMed
-
- Edinger M, et al. CD4+CD25+ regulatory T cells preserve graft-versus-tumor activity while inhibiting graft-versus-host disease after bone marrow transplantation. Nat. Med. 2003;9:1144–1150. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
