

IL-6 and CD8+ T cell counts combined are an early predictor of in-hospital mortality of patients with COVID-19
- PMID: 32544099
- PMCID: PMC7406244
- DOI: 10.1172/jci.insight.139024
IL-6 and CD8+ T cell counts combined are an early predictor of in-hospital mortality of patients with COVID-19
Abstract
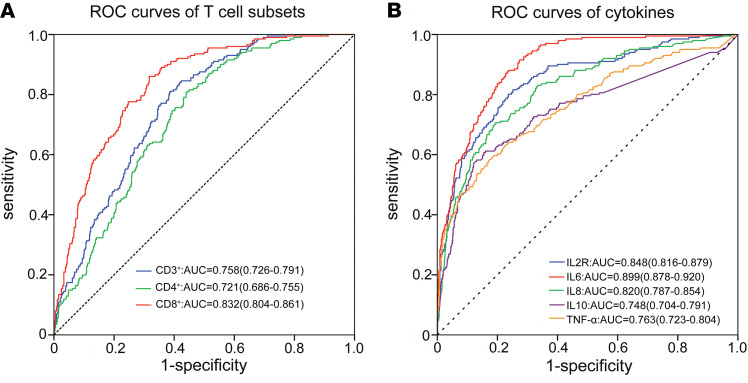
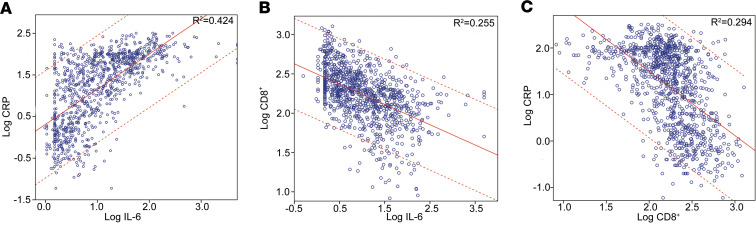
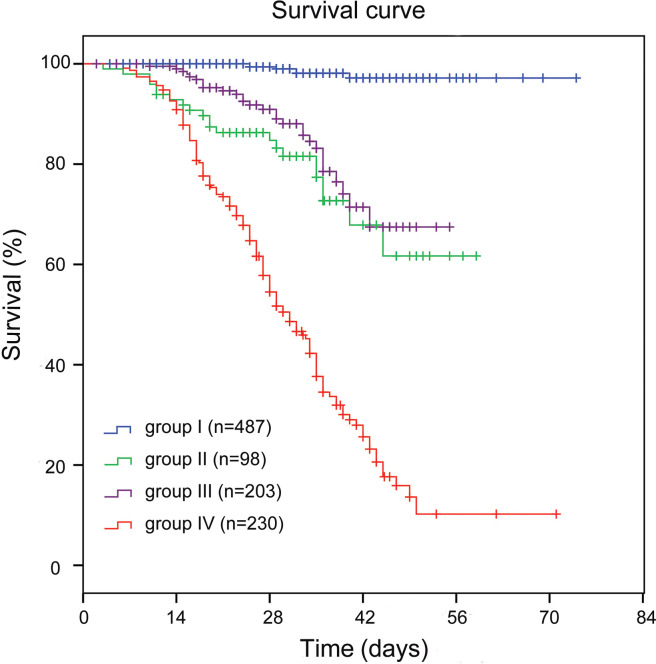
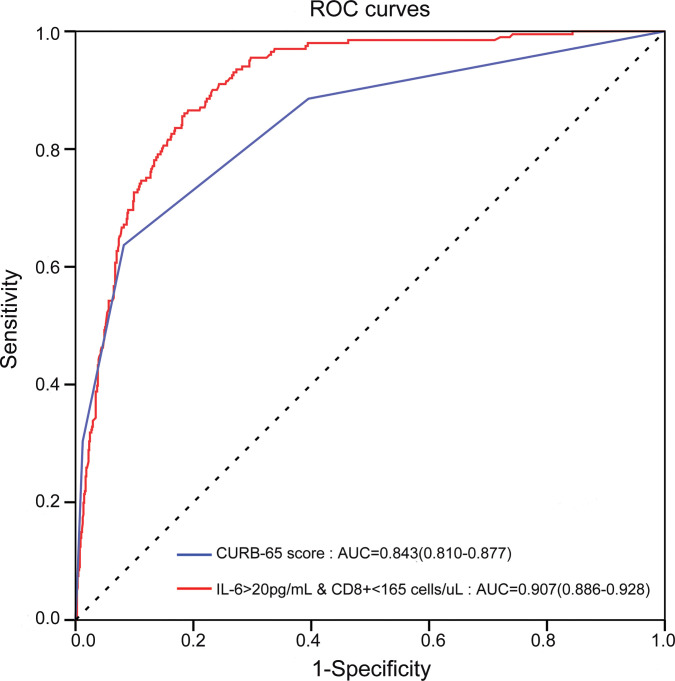
BACKGROUNDFatal cases of COVID-19 are increasing globally. We retrospectively investigated the potential of immunologic parameters as early predictors of COVID-19.METHODSA total of 1018 patients with confirmed COVID-19 were enrolled in our 2-center retrospective study. Clinical feature, laboratory test, immunological test, radiological findings, and outcomes data were collected. Univariate and multivariable logistic regression analyses were performed to evaluate factors associated with in-hospital mortality. Receiver operator characteristic (ROC) curves and survival curves were plotted to evaluate their clinical utility.RESULTSThe counts of all T lymphocyte subsets were markedly lower in nonsurvivors than in survivors, especially CD8+ T cells. Among all tested cytokines, IL-6 was elevated most significantly, with an upward trend of more than 10-fold. Using multivariate logistic regression analysis, IL-6 levels of more than 20 pg/mL and CD8+ T cell counts of less than 165 cells/μL were found to be associated with in-hospital mortality after adjusting for confounding factors. Groups with IL-6 levels of more than 20 pg/mL and CD8+ T cell counts of less than 165 cells/μL had a higher percentage of older and male patients as well as a higher proportion of patients with comorbidities, ventilation, intensive care unit admission, shock, and death. Furthermore, the receiver operating curve of the model combining IL-6 (>20 pg/mL) and CD8+ T cell counts (<165 cells/μL) displayed a more favorable discrimination than that of the CURB-65 score. The Hosmer-Lemeshow test showed a good fit of the model, with no statistical significance.CONCLUSIONIL-6 (>20 pg/mL) and CD8+ T cell counts (<165 cells/μL) are 2 reliable prognostic indicators that accurately stratify patients into risk categories and predict COVID-19 mortality.FundingThis work was supported by funding from the National Natural Science Foundation of China (no. 81772477 and 81201848).
Keywords: Cytokines; Infectious disease; Pulmonology; T cells.
Conflict of interest statement
Figures
Similar articles
-
Abnormal immunity of non-survivors with COVID-19: predictors for mortality.Infect Dis Poverty. 2020 Aug 3;9(1):108. doi: 10.1186/s40249-020-00723-1. Infect Dis Poverty. 2020. PMID: 32746940 Free PMC article.
-
Suppressed T cell-mediated immunity in patients with COVID-19: A clinical retrospective study in Wuhan, China.J Infect. 2020 Jul;81(1):e51-e60. doi: 10.1016/j.jinf.2020.04.012. Epub 2020 Apr 18. J Infect. 2020. PMID: 32315725 Free PMC article.
-
Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients.EBioMedicine. 2020 May;55:102763. doi: 10.1016/j.ebiom.2020.102763. Epub 2020 Apr 18. EBioMedicine. 2020. PMID: 32361250 Free PMC article.
-
Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis.Clin Chem Lab Med. 2020 Jun 25;58(7):1021-1028. doi: 10.1515/cclm-2020-0369. Clin Chem Lab Med. 2020. PMID: 32286245 Review.
-
Lymphocyte Subset Counts in COVID-19 Patients: A Meta-Analysis.Cytometry A. 2020 Aug;97(8):772-776. doi: 10.1002/cyto.a.24172. Epub 2020 Jul 18. Cytometry A. 2020. PMID: 32542842 Free PMC article. Review.
Cited by
-
In Silico Analysis Predicts a Limited Impact of SARS-CoV-2 Variants on CD8 T Cell Recognition.Front Immunol. 2022 Apr 27;13:891524. doi: 10.3389/fimmu.2022.891524. eCollection 2022. Front Immunol. 2022. PMID: 35572563 Free PMC article.
-
The Role of SARS-CoV-2 Nucleocapsidic Antigen and Krebs von den Lungen 6 Serum Levels in Predicting COVID-19 Pneumonia Outcome.Diagnostics (Basel). 2024 Mar 18;14(6):642. doi: 10.3390/diagnostics14060642. Diagnostics (Basel). 2024. PMID: 38535062 Free PMC article.
-
Recuperative herbal formula Jing Si maintains vasculature permeability balance, regulates inflammation and assuages concomitants of "Long-Covid".Biomed Pharmacother. 2023 Jul;163:114752. doi: 10.1016/j.biopha.2023.114752. Epub 2023 Apr 26. Biomed Pharmacother. 2023. PMID: 37116351 Free PMC article.
-
Macrophage Boolean networks in the time of SARS-CoV-2.Front Immunol. 2022 Oct 17;13:997434. doi: 10.3389/fimmu.2022.997434. eCollection 2022. Front Immunol. 2022. PMID: 36325317 Free PMC article. No abstract available.
-
Clinical prediction models in hospitalized patients with COVID-19: A multicenter cohort study.Respir Med. 2022 Oct;202:106954. doi: 10.1016/j.rmed.2022.106954. Epub 2022 Aug 21. Respir Med. 2022. PMID: 36057141 Free PMC article.
References
-
- Chen L, et al. [Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia] Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(3):203–208. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
