

Review
doi: 10.1164/rccm.202004-1263PP.
Coughs and Sneezes: Their Role in Transmission of Respiratory Viral Infections, Including SARS-CoV-2
Affiliations
- PMID: 32543913
- PMCID: PMC7462404
- DOI: 10.1164/rccm.202004-1263PP
Item in Clipboard
Review
Coughs and Sneezes: Their Role in Transmission of Respiratory Viral Infections, Including SARS-CoV-2
Am J Respir Crit Care Med.
.
No abstract available
Figures
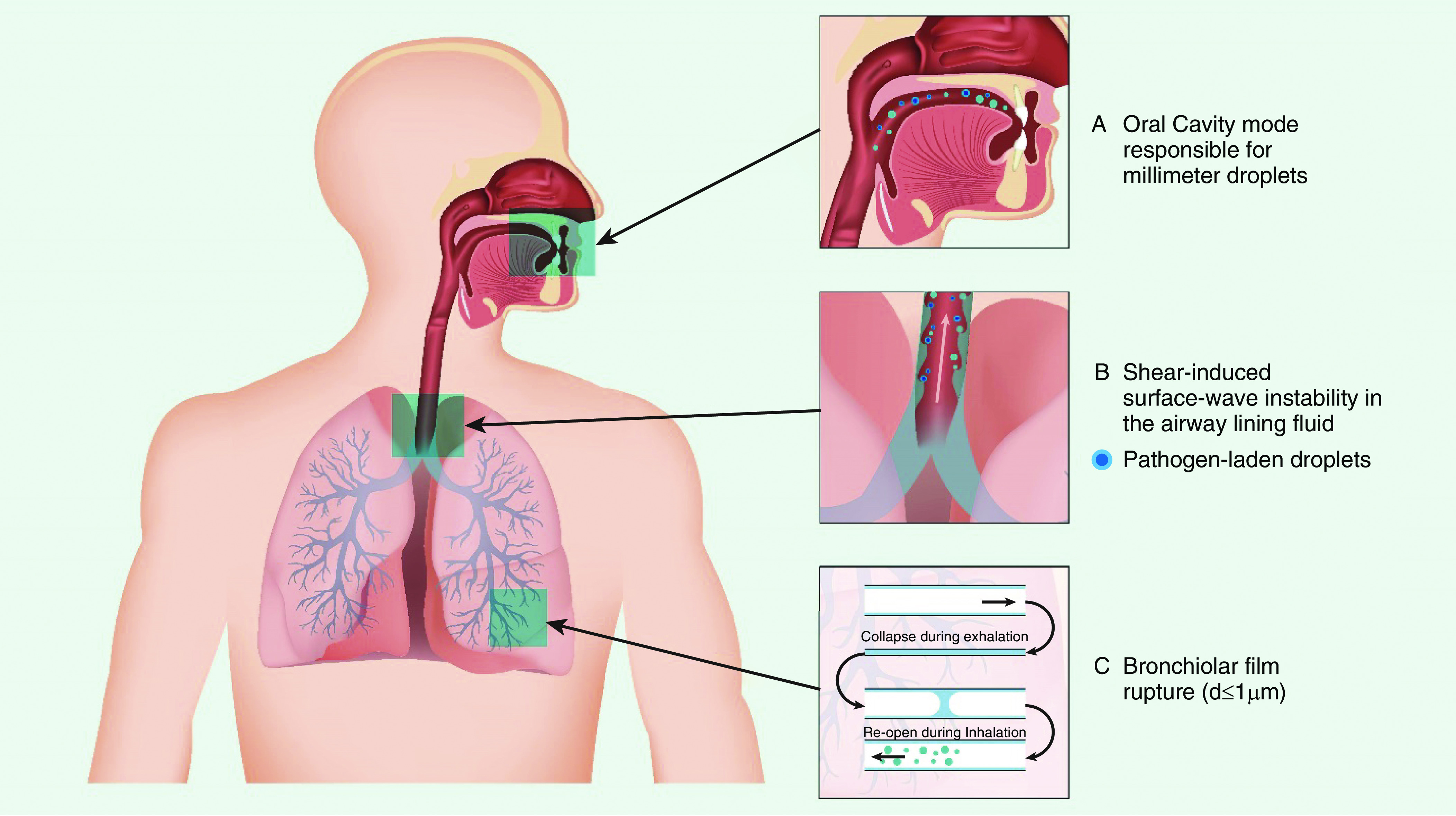
Schematic showing the site of origin and mechanisms of droplet generation from the respiratory tract. Adapted by permission from Reference .
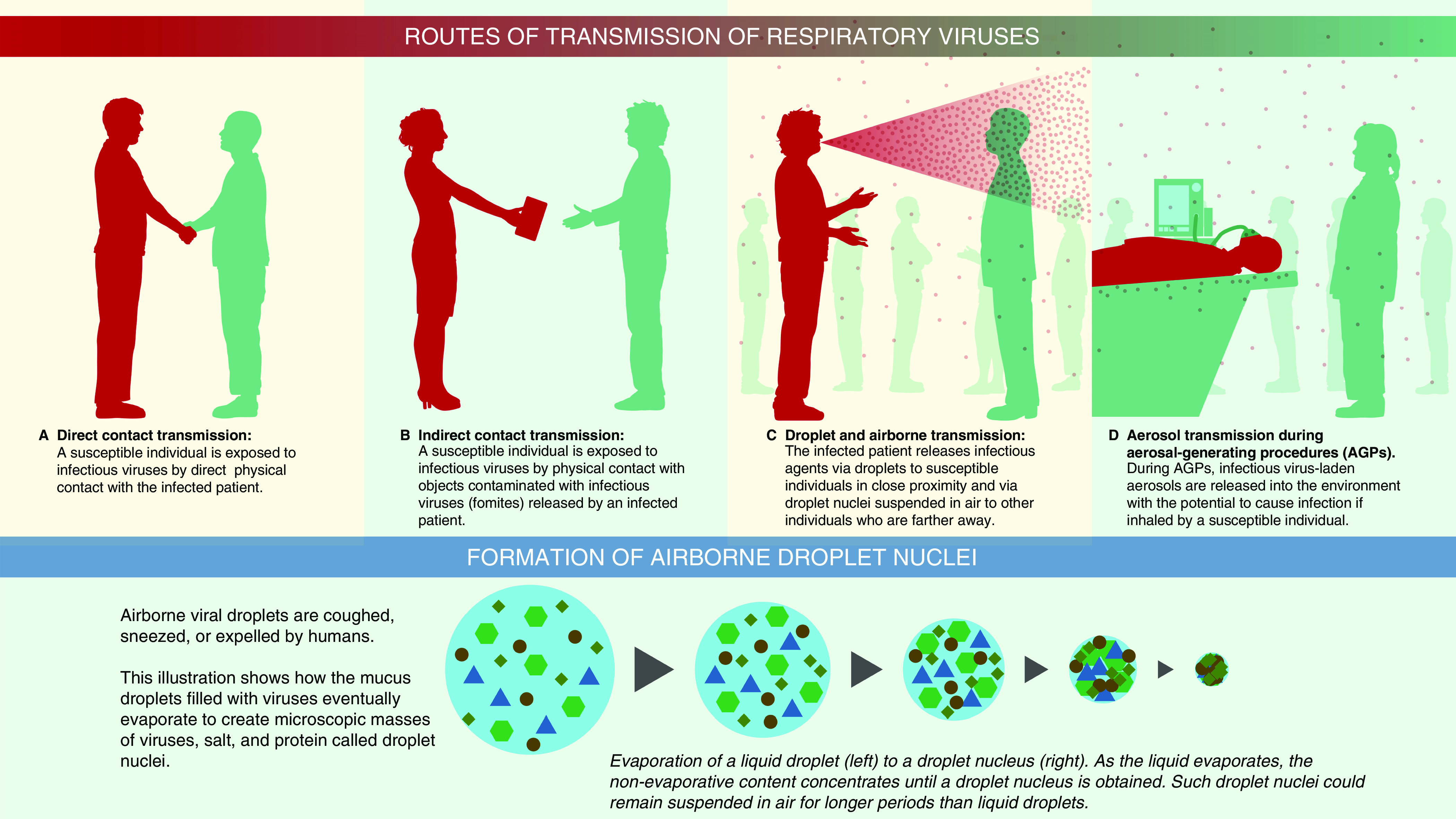
Illustration to show various routes of transmission. For contact transmission, an infected person can transfer virus-laden respiratory secretions by (A) direct physical contact or (B) indirectly. If an infected person sneezes or coughs and droplets deposit or if they have the virus on their hands from touching their face or blowing their nose and then touch an object or surface, then that object or surface serves as a repository for the contagion. When another individual touches the same object or surface that has the virus on it and then touches their mouth, nose, or eyes, the virus is transmitted to these mucosal surfaces. The most common mode of spread for respiratory viruses is via (C) respiratory droplet transmission. Virus-laden droplets (generated by coughing, sneezing, or talking) are propelled from an infected person directly onto the mucosal surfaces of a host. Respiratory droplets are larger and generally fall to the ground after traveling short distances. Transmission of infection can also occur indirectly after the infected droplets have deposited if a host touches the contaminated surface and then touches their face. (C) Airborne transmission occurs when virus-laden fine respiratory droplets remain viable in the environment and are inhaled by a susceptible individual. This transmission can occur either directly by inhalation of fine droplets expelled from (C) an infected person or (D) during aerosol-generating procedures on an infected individual. Larger droplets expelled by coughing or sneezing evaporate, and these smaller and drier droplet nuclei containing infective microorganisms (lower panel) remain suspended in air for extended periods. They have the potential to deposit in the lower respiratory tract after they are inhaled. Larger droplet nuclei that settle out from the air can potentially be resuspended after their size decreases from evaporation, in combination with an aerosol-generating activity such as making a bed or while doffing personal protective equipment.
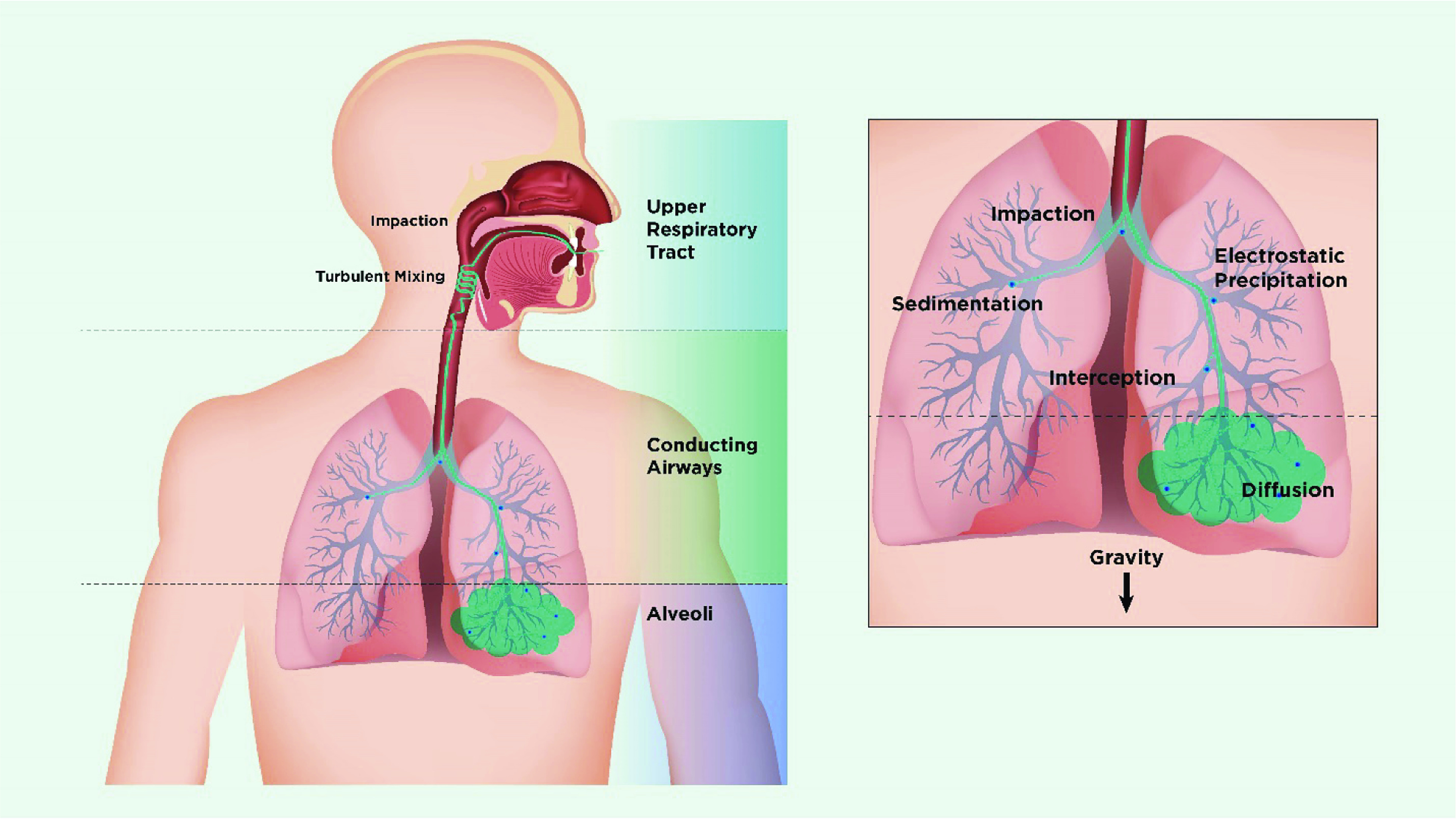
Schematic showing mechanisms of deposition of inhaled particles in the lung. On entering the nasal or oral cavity, particles deposit by impaction, turbulent mixing, sedimentation, and Brownian motion depending on their size. Particles >5 μm in aerodynamic diameter are most likely to deposit by impaction in the oropharynx and be swallowed, whereas particles <5 μm have the greatest potential for lung deposition. Particles between 4 and 5 μm deposit primarily in the bronchial/conducting airways, whereas smaller particles remain suspended in the airstream and penetrate to the peripheral airways and alveoli. In the lung periphery, a significant reduction in airflow rate allows particles to deposit predominantly by sedimentation, with gravity causing them to “rain out” and deposit. Most particles between 0.1 and 1 μm diffuse by Brownian motion and deposit when they collide with the airway wall. The longer the residence time in the smaller, peripheral airways, the greater the deposition from sedimentation and Brownian motion processes. Inhaled particles that do not deposit are exhaled. Adapted by permission from Reference .
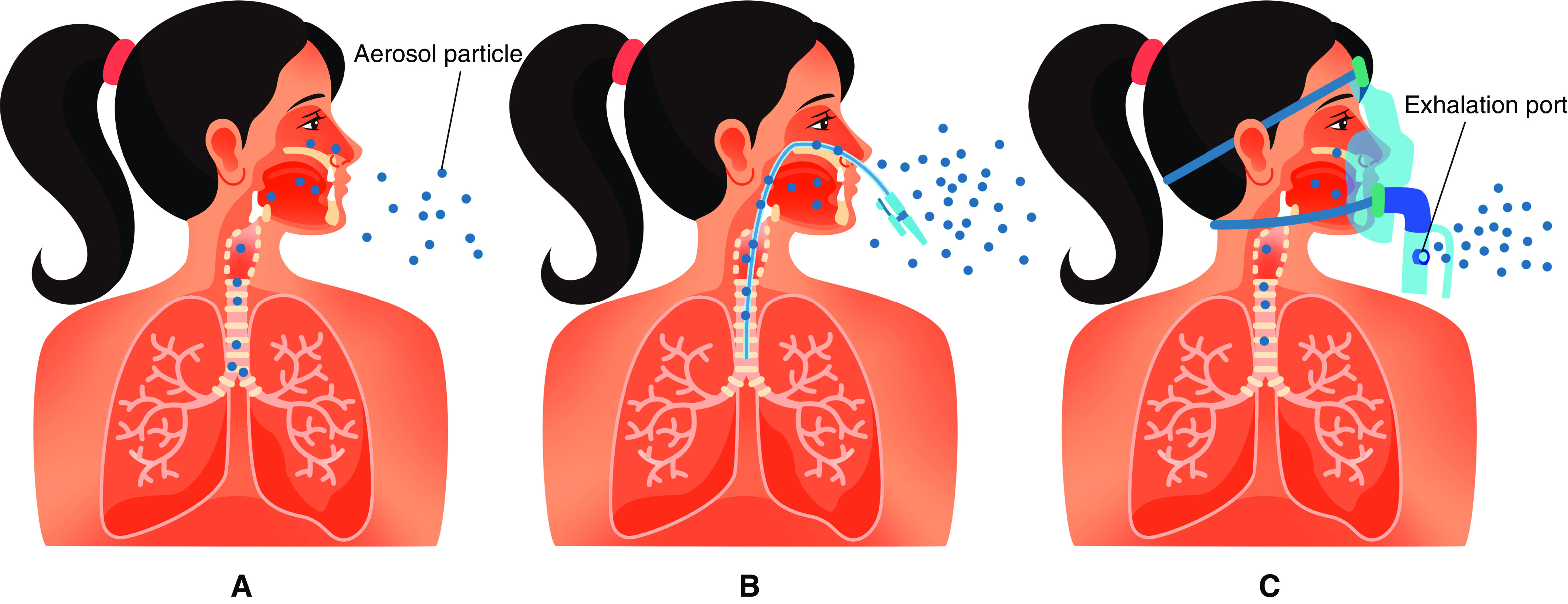
Illustration to show the difference between aerosol “generating” versus aerosol “dispersing” procedures. A shows that a small amount of aerosols generated during normal breathing travel short distances before evaporation. B shows a burst of aerosols generated during procedures that provoke coughing such as suctioning, intubation, or bronchoscopy. In C, administration of therapeutic aerosols by nebulizer, noninvasive ventilation, or use of high-flow nasal cannula could disperse aerosols from the patient as a jet to a greater distance.
Similar articles
-
Extracorporeal Membrane Oxygenation for COVID-19.Innovations (Phila). 2020 Jul/Aug;15(4):306-313. doi: 10.1177/1556984520937821. Epub 2020 Jul 21. Innovations (Phila). 2020. PMID: 32692258 No abstract available.
-
Changes in the work mode of cardiologists during the COVID-19 epidemic in Wuhan.Eur Heart J. 2020 Aug 1;41(29):2729-2730. doi: 10.1093/eurheartj/ehaa424. Eur Heart J. 2020. PMID: 32406507 Free PMC article. No abstract available.
-
Points & Pearls: Novel 2019 Coronavirus SARS-CoV-2 (COVID-19) An Overview for Emergency Clinicians.Emerg Med Pract. 2020 May 1;22(5):e1-e2. Emerg Med Pract. 2020. PMID: 32421272 Review. No abstract available.
-
Moving Personal Protective Equipment Into the Community: Face Shields and Containment of COVID-19.JAMA. 2020 Jun 9;323(22):2252-2253. doi: 10.1001/jama.2020.7477. JAMA. 2020. PMID: 32347911 No abstract available.
-
COVID-19: How Do We Stay Safe?Am J Respir Crit Care Med. 2020 Sep 1;202(5):P15-P16. doi: 10.1164/rccm.2025P15. Am J Respir Crit Care Med. 2020. PMID: 32870036 Review. No abstract available.
Cited by
-
Letter to the Editor Regarding "Pre-HCT Lung Computed Tomography as an Alternative to PFT During the COVID-19 Pandemic".Transplant Cell Ther. 2021 Feb;27(2):188-189. doi: 10.1016/j.jtct.2020.10.019. Epub 2020 Dec 11. Transplant Cell Ther. 2021. PMID: 33830038 Free PMC article. No abstract available.
-
Real-World Evidence on the Effectiveness of Plexiglass Barriers in Reducing Aerosol Exposure.Pathog Immun. 2022 Nov 4;7(2):66-77. doi: 10.20411/pai.v7i2.533. eCollection 2022. Pathog Immun. 2022. PMID: 36381131 Free PMC article.
-
Survival of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Herpes Simplex Virus 1 (HSV-1) on Foods Stored at Refrigerated Temperature.Foods. 2021 May 4;10(5):1005. doi: 10.3390/foods10051005. Foods. 2021. PMID: 34064494 Free PMC article.
-
High-Flow Aerosol-Dispersing versus Aerosol-Generating Procedures.Am J Respir Crit Care Med. 2020 Oct 15;202(8):1069-1071. doi: 10.1164/rccm.202008-3317ED. Am J Respir Crit Care Med. 2020. PMID: 32877201 Free PMC article. No abstract available.
-
Effect of SARS-CoV-2 infection on asthma patients.Front Med (Lausanne). 2022 Aug 2;9:928637. doi: 10.3389/fmed.2022.928637. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35983093 Free PMC article.
References
-
- Fitzgerald D, Sterling TR, Haas D.Mycobacterium tuberculosis Bennett JE, Dolin R, Blaser MJ.editors. Mandell, Douglas, and Bennett's principles and practice of infectious diseases; 9th ed.Philadelphia: Elsevier; 20202985–3021.
-
- Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008;371:1364–1374. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
