

Dynamic impact of transfusion ratios on outcomes in severely injured patients: Targeted machine learning analysis of the Pragmatic, Randomized Optimal Platelet and Plasma Ratios randomized clinical trial
- PMID: 32520897
- PMCID: PMC7830749
- DOI: 10.1097/TA.0000000000002819
Dynamic impact of transfusion ratios on outcomes in severely injured patients: Targeted machine learning analysis of the Pragmatic, Randomized Optimal Platelet and Plasma Ratios randomized clinical trial
Abstract
Background: Massive transfusion protocols to treat postinjury hemorrhage are based on predefined blood product transfusion ratios followed by goal-directed transfusion based on patient's clinical evolution. However, it remains unclear how these transfusion ratios impact patient outcomes over time from injury.
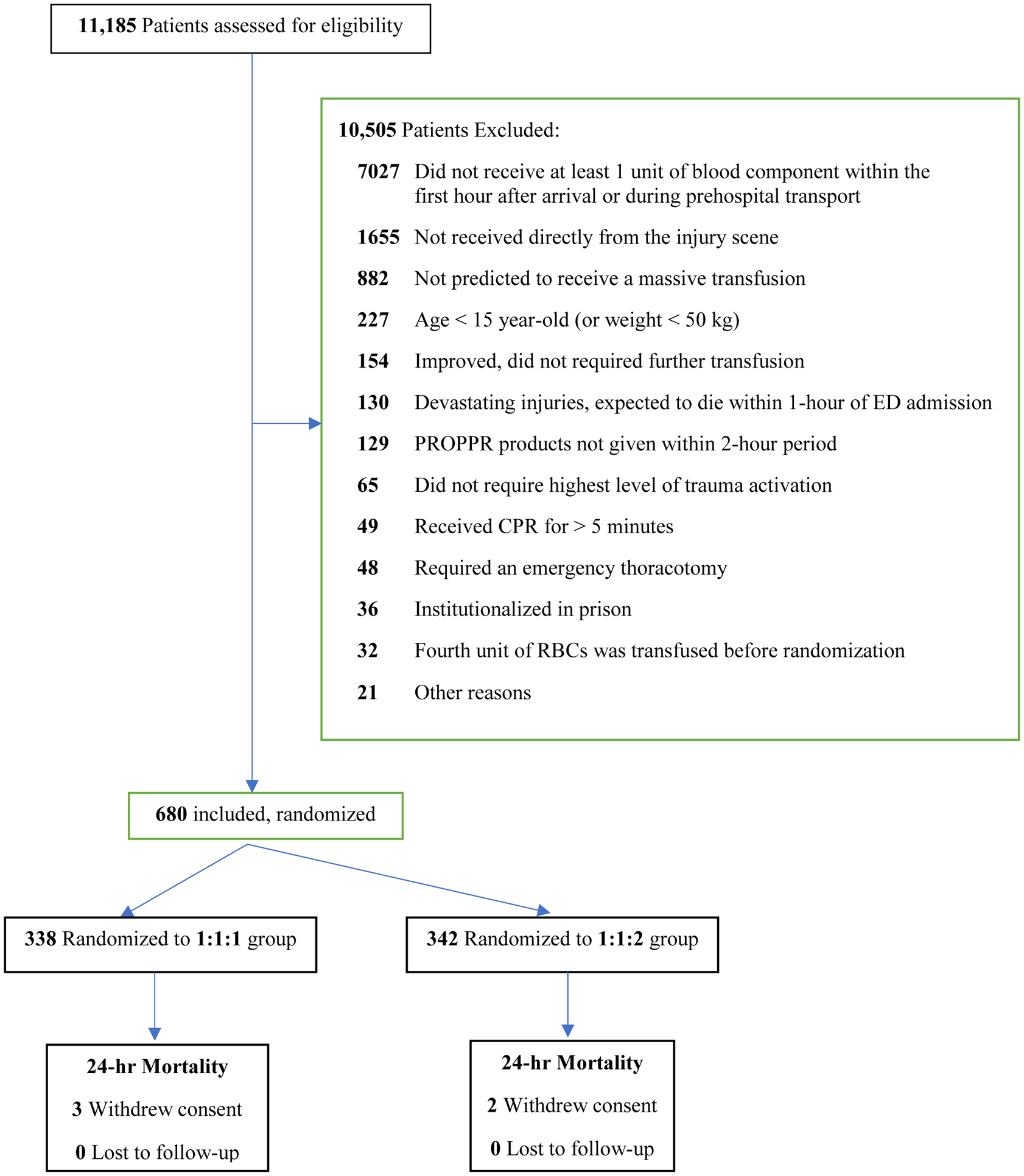
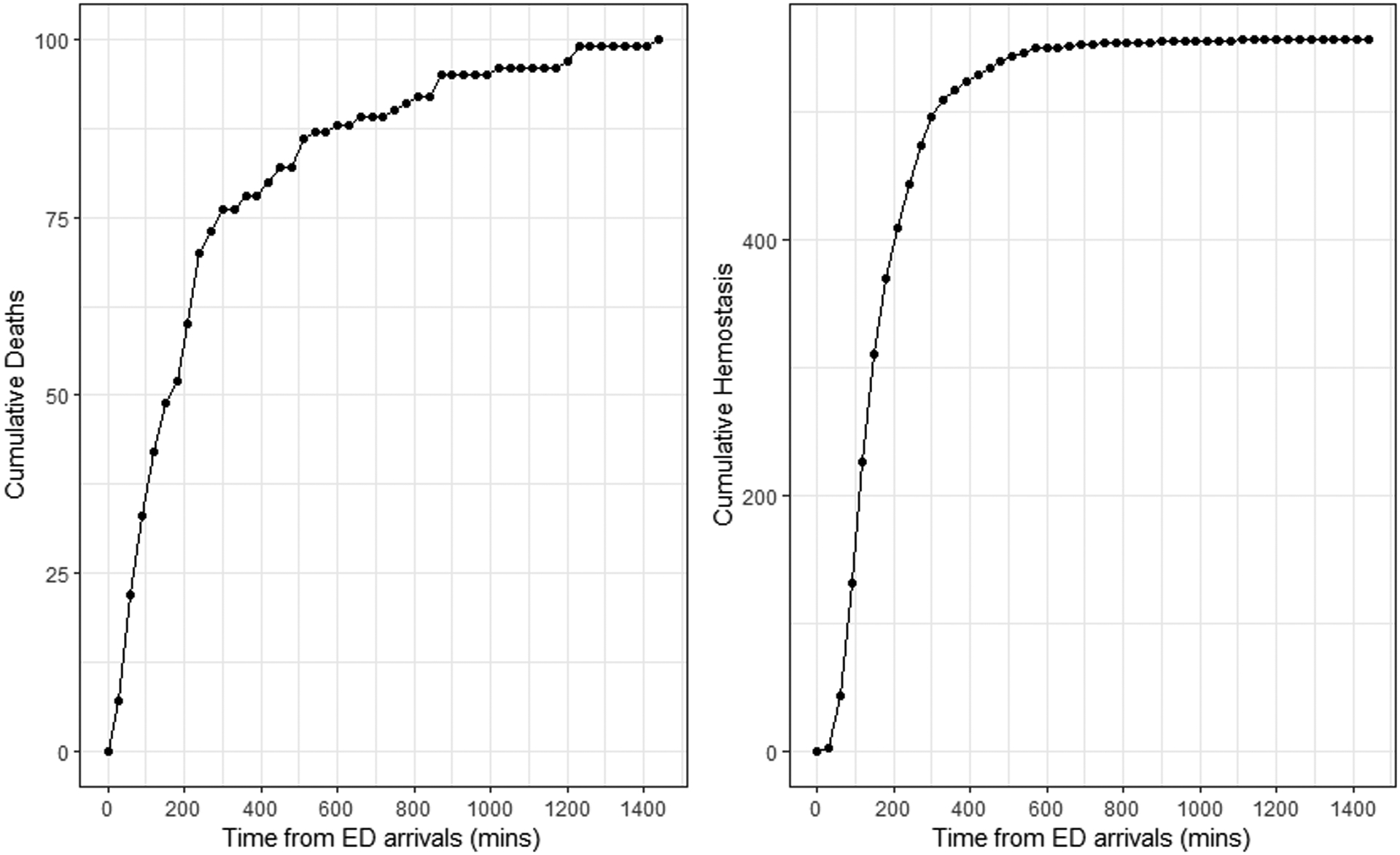
Methods: The Pragmatic, Randomized Optimal Platelet and Plasma Ratios (PROPPR) is a phase 3, randomized controlled trial, across 12 Level I trauma centers in North America. From 2012 to 2013, 680 severely injured patients required massive transfusion. We used semiparametric machine learning techniques and causal inference methods to augment the intent-to-treat analysis of PROPPR, estimating the dynamic relationship between transfusion ratios and outcomes: mortality and hemostasis at different timepoints during the first 24 hours after admission.
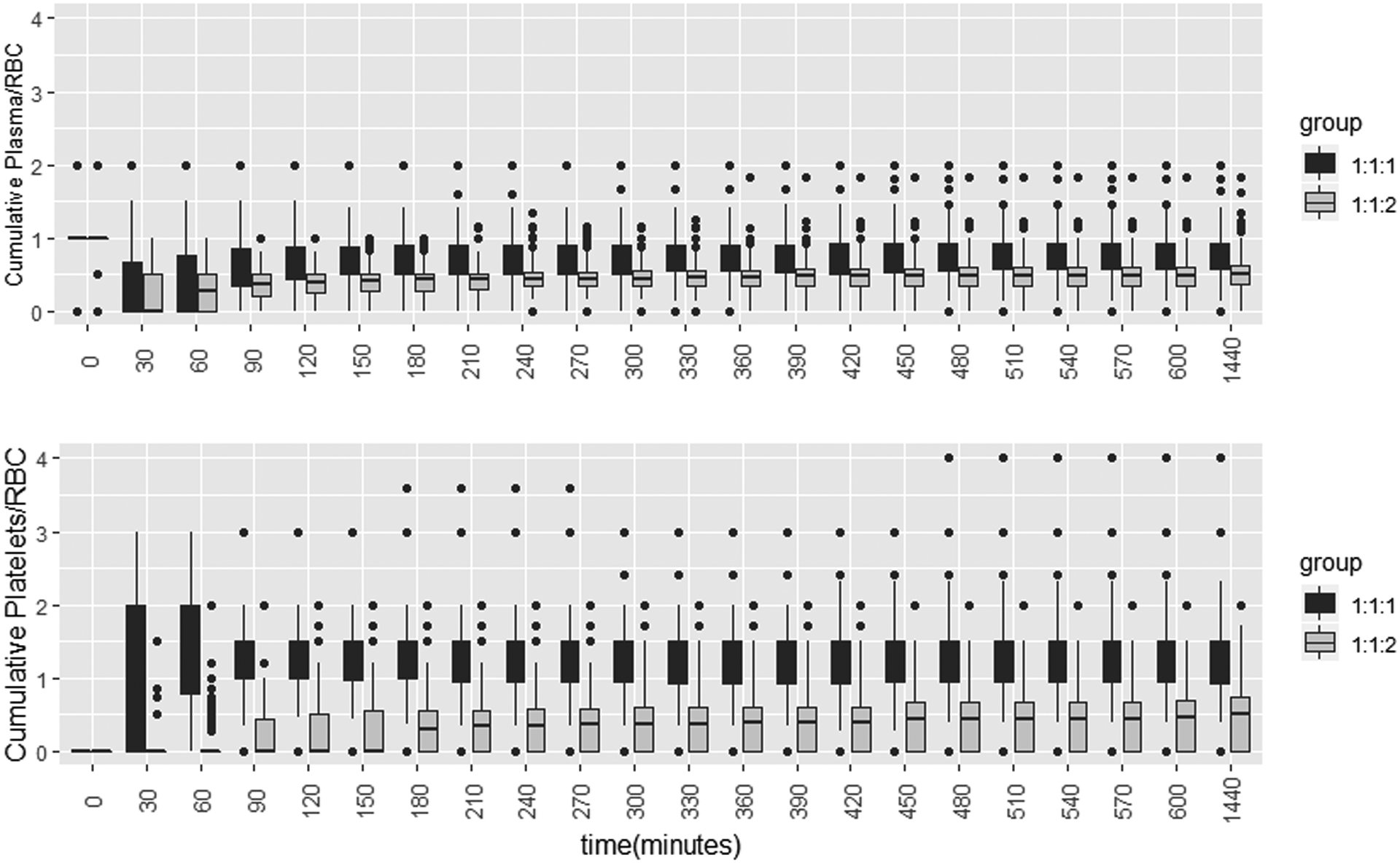
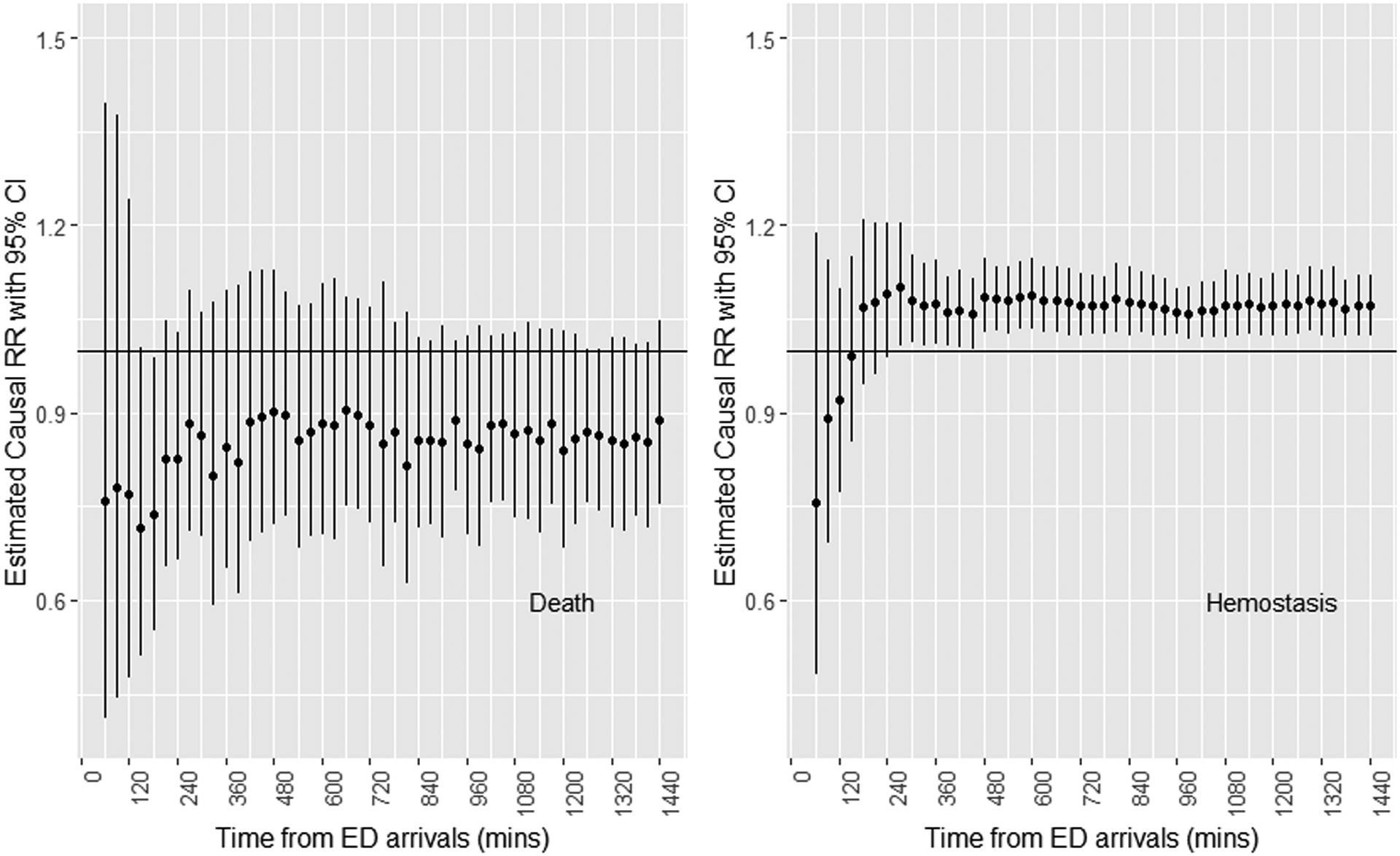
Results: In the intention-to-treat analysis, the 1:1:1 group tended to have decreased mortality, but with no statistical significance. For patients in whom hemostasis took longer than 2 hours, the 1:1:1 ratio was associated with a higher probability of hemostasis, statistically significant from the 4 hour on. In the per-protocol, actual-transfusion-ratios-received analysis, during four successive time intervals, no significant association was found between the actual ratios and mortality. When comparing patient groups who received both high plasma/PRBC and high platelet/PRBC ratios to the group of low ratios in both, the relative risk of achieving hemostasis was 2.49 (95% confidence interval, 1.19-5.22) during the third hour after admission, suggesting a significant beneficial impact of higher transfusion ratios of plasma and platelets on hemostasis.
Conclusion: Our results suggest that the impact of transfusion ratios on hemostasis is dynamic. Overall, the transfusion ratios had no significant impact on mortality over time. However, receiving higher ratios of platelets and plasma relative to red blood cells hastens hemostasis in subjects who have yet to achieve hemostasis within 3 hours after hospital admission.
Level of evidence: Therapeutic IV.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial.JAMA. 2015 Feb 3;313(5):471-82. doi: 10.1001/jama.2015.12. JAMA. 2015. PMID: 25647203 Free PMC article. Clinical Trial.
-
Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) Trial: design, rationale and implementation.Injury. 2014 Sep;45(9):1287-95. doi: 10.1016/j.injury.2014.06.001. Epub 2014 Jun 10. Injury. 2014. PMID: 24996573 Free PMC article. Clinical Trial.
-
Platelet transfusions improve hemostasis and survival in a substudy of the prospective, randomized PROPPR trial.Blood Adv. 2018 Jul 24;2(14):1696-1704. doi: 10.1182/bloodadvances.2018017699. Blood Adv. 2018. PMID: 30030268 Free PMC article. Clinical Trial.
-
Massive transfusion protocol in adult trauma population.Am J Emerg Med. 2020 Dec;38(12):2661-2666. doi: 10.1016/j.ajem.2020.07.041. Epub 2020 Jul 22. Am J Emerg Med. 2020. PMID: 33071074 Review.
-
Massive transfusion: red blood cell to plasma and platelet unit ratios for resuscitation of massive hemorrhage.Curr Opin Hematol. 2015 Nov;22(6):533-9. doi: 10.1097/MOH.0000000000000184. Curr Opin Hematol. 2015. PMID: 26390160 Review.
Cited by
-
Machine learning in transfusion medicine: A scoping review.Transfusion. 2024 Jan;64(1):162-184. doi: 10.1111/trf.17582. Epub 2023 Nov 10. Transfusion. 2024. PMID: 37950535 Free PMC article. Review. No abstract available.
-
Machine learning in perioperative medicine: a systematic review.J Anesth Analg Crit Care. 2022 Jan 15;2(1):2. doi: 10.1186/s44158-022-00033-y. J Anesth Analg Crit Care. 2022. PMID: 37386544 Free PMC article. Review.
-
Survival and neurologic outcomes following aortic occlusion for trauma and hemorrhagic shock in a hybrid operating room.World J Emerg Surg. 2023 Mar 23;18(1):21. doi: 10.1186/s13017-023-00484-w. World J Emerg Surg. 2023. PMID: 36959585 Free PMC article.
-
The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition.Crit Care. 2023 Mar 1;27(1):80. doi: 10.1186/s13054-023-04327-7. Crit Care. 2023. PMID: 36859355 Free PMC article. Review.
-
Survival and neurologic outcomes following aortic occlusion for trauma and hemorrhagic shock in a hybrid operating room.Res Sq [Preprint]. 2023 Jan 13:rs.3.rs-2459030. doi: 10.21203/rs.3.rs-2459030/v1. Res Sq. 2023. Update in: World J Emerg Surg. 2023 Mar 23;18(1):21. doi: 10.1186/s13017-023-00484-w. PMID: 36711502 Free PMC article. Updated. Preprint.
References
-
- Heron M Deaths: Leading Causes for 2015. National Vital Statistics Reports, 66(5), 2017. Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr66/nvsr66_05.pdf. Accessed December 18, 2019. - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE; Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–482. - PMC - PubMed
-
- Cotton BA, Reddy N, Hatch QM, LeFebvre E, Wade CE, Kozar RA, Gill BS, Albarado R, McNutt MK, Holcomb JB. Damage control resuscitation is associated with a reduction in resuscitation volumes and improvement in survival in 390 damage control laparotomy patients. Ann Surg. 2011;254(4):598–605. - PMC - PubMed
-
- Langan NR, Eckert M, Martin MJ. Changing patterns of in-hospital deaths following implementation of damage control resuscitation practices in us forward military treatment facilities. JAMA Surg. 2014;149(9):904–912. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
