

Multi-parametric arterial spin labelling and diffusion-weighted magnetic resonance imaging in differentiation of grade II and grade III gliomas
- PMID: 32467745
- PMCID: PMC7247019
- DOI: 10.5114/pjr.2020.93397
Multi-parametric arterial spin labelling and diffusion-weighted magnetic resonance imaging in differentiation of grade II and grade III gliomas
Abstract
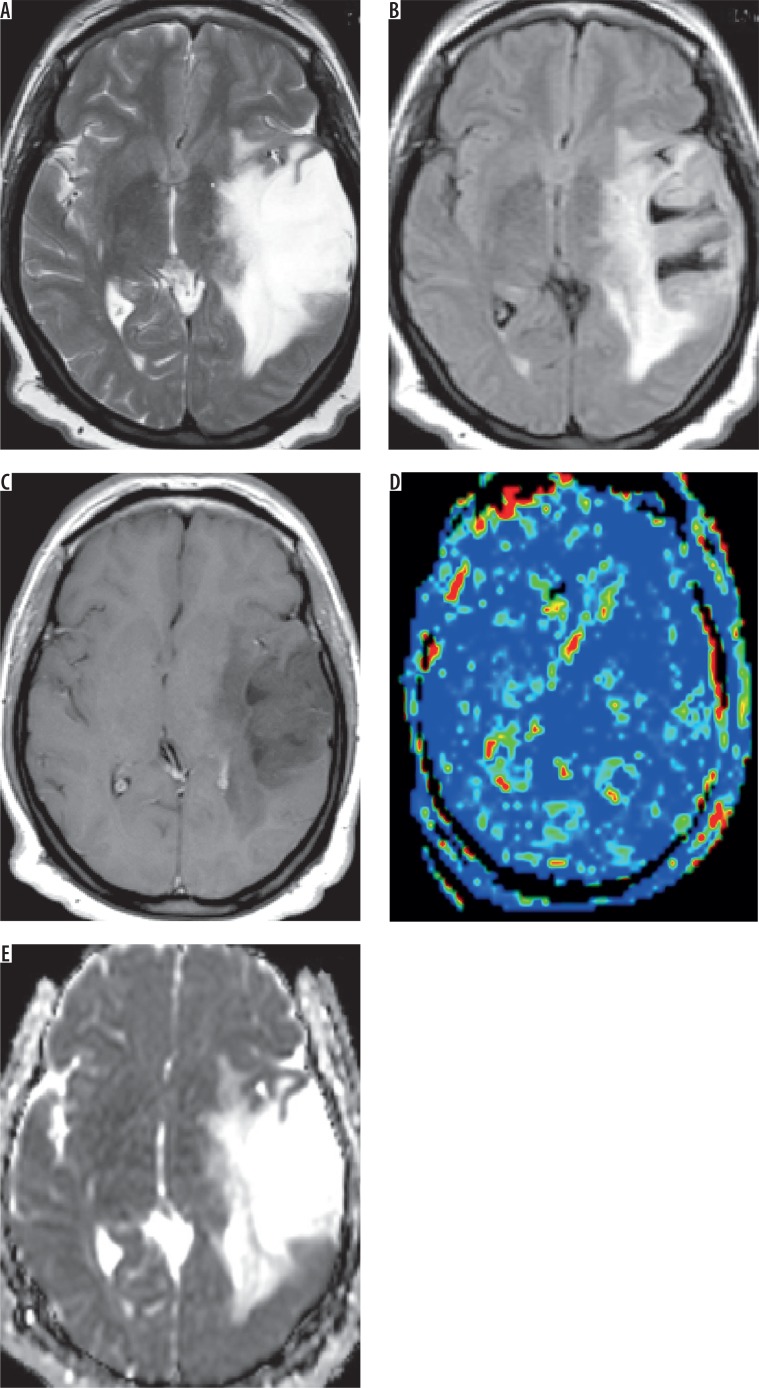
Purpose: To assess arterial spin labelling (ASL) perfusion and diffusion MR imaging (DWI) in the differentiation of grade II from grade III gliomas.
Material and methods: A prospective cohort study was done on 36 patients (20 male and 16 female) with diffuse gliomas, who underwent ASL and DWI. Diffuse gliomas were classified into grade II and grade III. Calculation of tumoural blood flow (TBF) and apparent diffusion coefficient (ADC) of the tumoral and peritumoural regions was made. The ROC curve was drawn to differentiate grade II from grade III gliomas.
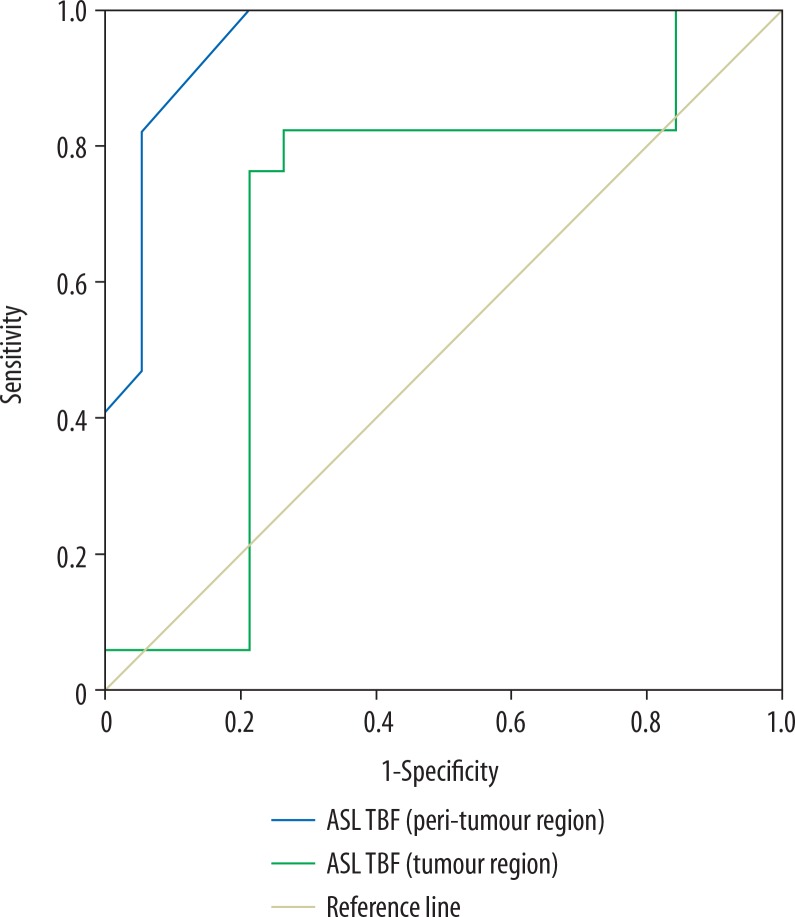
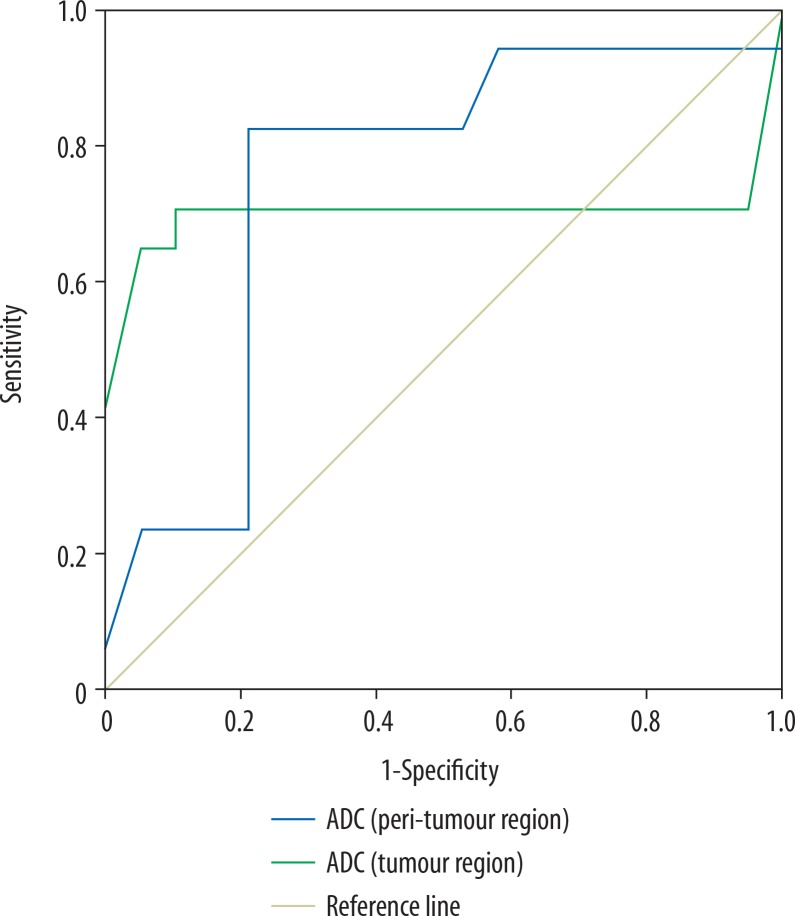
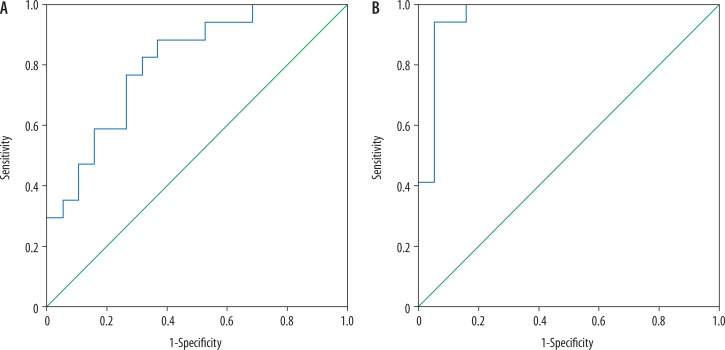
Results: There was a significant difference in TBF of tumoural and peritumoural regions of grade II and III gliomas (p = 0.02 and p =0.001, respectively). Selection of 26.1 and 14.8 ml/100 g/min as the cut-off for TBF of tumoural and peritumoural regions differentiated between both groups with area under curve (AUC) of 0.69 and 0.957, and accuracy of 77.8% and 88.9%, respectively. There was small but significant difference in the ADC of tumoural and peritumoural regions between grade II and III gliomas (p = 0.02 for both). The selection of 1.06 and 1.36 × 10-3 mm2/s as the cut-off of ADC of tumoural and peritumoural regions was made, to differentiate grade II from III with AUC of 0.701 and 0.748, and accuracy of 80.6% and 80.6%, respectively. Combined TBF and ADC of tumoural regions revealed an AUC of 0.808 and accuracy of 72.7%. Combined TBF and ADC for peritumoural regions revealed an AUC of 0.96 and accuracy of 94.4%.
Conclusion: TBF and ADC of tumoural and peritumoural regions are accurate non-invasive methods of differentiation of grade II from grade III gliomas.
Keywords: arterial spin labelling; diffusion weighted imaging; glioma; grading.
Copyright © Polish Medical Society of Radiology 2020.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Multi-parametric MR imaging using pseudo-continuous arterial-spin labeling and diffusion-weighted MR imaging in differentiating subtypes of parotid tumors.Magn Reson Imaging. 2019 Nov;63:55-59. doi: 10.1016/j.mri.2019.08.005. Epub 2019 Aug 15. Magn Reson Imaging. 2019. PMID: 31422165
-
Combination of three-dimensional arterial spin labeling and stretched-exponential model in grading of gliomas.Medicine (Baltimore). 2019 Jun;98(25):e16012. doi: 10.1097/MD.0000000000016012. Medicine (Baltimore). 2019. PMID: 31232933 Free PMC article.
-
Intravoxel incoherent motion diffusion-weighted imaging analysis of diffusion and microperfusion in grading gliomas and comparison with arterial spin labeling for evaluation of tumor perfusion.J Magn Reson Imaging. 2016 Sep;44(3):620-32. doi: 10.1002/jmri.25191. Epub 2016 Feb 16. J Magn Reson Imaging. 2016. PMID: 26880230
-
Multi-parametric arterial spin labeling and diffusion-weighted imaging of paranasal sinuses masses.Oral Radiol. 2023 Apr;39(2):321-328. doi: 10.1007/s11282-022-00640-z. Epub 2022 Jul 28. Oral Radiol. 2023. PMID: 35900660
-
Measurements of diagnostic examination performance using quantitative apparent diffusion coefficient and proton MR spectroscopic imaging in the preoperative evaluation of tumor grade in cerebral gliomas.Eur J Radiol. 2011 Nov;80(2):462-70. doi: 10.1016/j.ejrad.2010.07.017. Epub 2010 Aug 13. Eur J Radiol. 2011. PMID: 20708868
Cited by
-
Can Apparent Diffusion Coefficient Predict the Grade, Genotype, or Proliferation Index of Oligodendrogliomas.Asian J Neurosurg. 2021 Dec 18;16(4):752-758. doi: 10.4103/ajns.AJNS_520_20. eCollection 2021 Oct-Dec. Asian J Neurosurg. 2021. PMID: 35071073 Free PMC article.
-
Multimodal MRI-Based Radiomic Nomogram for the Early Differentiation of Recurrence and Pseudoprogression of High-Grade Glioma.Biomed Res Int. 2022 Sep 30;2022:4667117. doi: 10.1155/2022/4667117. eCollection 2022. Biomed Res Int. 2022. Retraction in: Biomed Res Int. 2023 Dec 29;2023:9869137. doi: 10.1155/2023/9869137 PMID: 36246986 Free PMC article. Retracted.
-
Association of dynamic susceptibility magnetic resonance imaging at initial tumor diagnosis with the prognosis of different molecular glioma subtypes.Neurol Sci. 2020 Dec;41(12):3625-3632. doi: 10.1007/s10072-020-04474-7. Epub 2020 May 28. Neurol Sci. 2020. PMID: 32462389 Free PMC article.
-
Radiotherapy in adult low-grade glioma: nationwide trends in treatment and outcomes.Clin Transl Oncol. 2021 Mar;23(3):628-637. doi: 10.1007/s12094-020-02458-9. Epub 2020 Jul 20. Clin Transl Oncol. 2021. PMID: 32691365
-
A Novel System for Precise Grading of Glioma.Bioengineering (Basel). 2022 Oct 7;9(10):532. doi: 10.3390/bioengineering9100532. Bioengineering (Basel). 2022. PMID: 36290500 Free PMC article.
References
-
- Van Den Bent MJ, Smits M, Kros JM, Chang SM. Diffuse infiltrating oligodendroglioma and astrocytoma. J Clin Oncol. 2017;35:2394–2401. - PubMed
-
- Delgado-López PD, Corrales-García EM, Martino J, Lastra-Aras E, Dueńas-Polo MT. Diffuse low-grade glioma: a review on the new molecular classification, natural history and current management strategies. Clin Transl Oncol. 2017;19:931–944. - PubMed
LinkOut - more resources
Full Text Sources