

Intrauterine insemination performance characteristics and post-processing total motile sperm count in relation to live birth for couples with unexplained infertility in a randomised, multicentre clinical trial
- PMID: 32432326
- PMCID: PMC7316499
- DOI: 10.1093/humrep/deaa027
Intrauterine insemination performance characteristics and post-processing total motile sperm count in relation to live birth for couples with unexplained infertility in a randomised, multicentre clinical trial
Abstract
Study question: Are intrauterine insemination (IUI) performance characteristics and post-processing total motile sperm count (TMC) related to live birth rate in couples with unexplained infertility?
Summary answer: Patient discomfort with IUI and lower inseminate TMC were associated with a reduced live birth rate, while time from hCG injection to IUI, sperm preparation method and ultrasound guidance for IUI were not associated with live birth success.
What is already known: We previously determined that some baseline characteristics of couples with unexplained infertility, including female age, duration of infertility, history of prior loss and income, were related to live birth rate across a course of ovarian stimulation and IUI treatment. However, the relationship between treatment outcomes and per-cycle characteristics, including ultrasound guidance for IUI, timing of IUI relative to hCG injection, difficult or painful IUI and inseminate TMC, are controversial, and most prior investigations have not evaluated live birth outcome.
Study design, size, duration: This was a secondary analyses of 2462 cycles from the Assessment of Multiple Intrauterine Gestations from Ovarian Stimulation (AMIGOS) clinical trial. This prospective, randomised, multicentre clinical trial determined live birth rates following IUI after ovarian stimulation with clomiphene citrate, letrozole or gonadotropins in 854 couples with unexplained infertility. It was conducted between 2011 and 2014, and couples could undergo up to four consecutive treatment cycles.
Participants/materials, setting, methods: AMIGOS was an NIH-sponsored Reproductive Medicine Network trial conducted at 12 clinical sites. Participants were women with unexplained infertility who were between 18 and 40 years of age. Cluster-weighted generalised estimating equations (GEE), which account for informative clustering of multiple IUI treatment cycles within the same patient, were used to determine associations between IUI performance characteristics, including inseminate TMC, and live birth rate. Efficiency curves were also generated to examine the relationship between inseminate TMC and live birth rate.
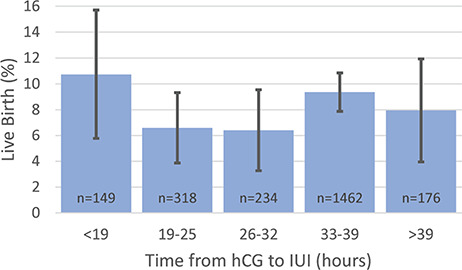
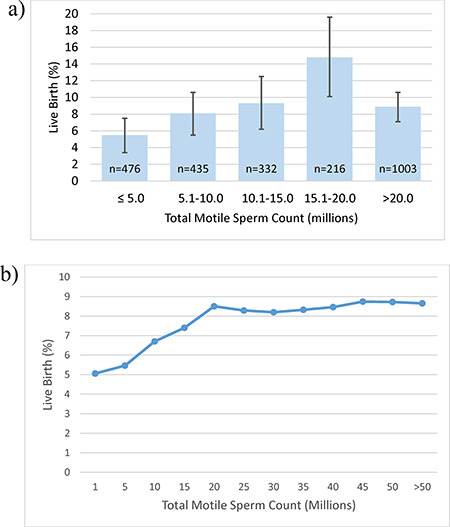
Main results and the role of chance: After adjustment for treatment group and baseline factors previously associated with live birth across a course of OS-IUI treatment, patient discomfort during the IUI procedure was associated with a reduction in live birth rate (aRR 0.40 (0.16-0.96)). Time from hCG trigger injection to IUI was not significantly associated with outcome. Higher TMC was associated with greater live birth rate (TMC 15.1-20.0 million (14.8%) compared to ≤5 million (5.5%)) (aRR 2.09 (1.31-3.33)). However, live births did occur with TMC ≤ 1 million (5.1%).
Limitations, reasons for caution: This investigation is a secondary analysis, and AMIGOS was not designed to address the present question. Since timed intercourse was allowed as part of the AMIGOS trial, we cannot rule out the possibility that any given pregnancy resulted from intercourse rather than IUI.
Wider implications of the findings: Most factors associated with the performance of IUI were not significantly related to obtaining live birth. Our findings suggest that higher TMC inseminated leads to an increase in live birth rate up to TMC ~20 million. However, there may be no reasonable threshold below which live birth is not possible with IUI.
Study funding/competing interest(s): Funding was received through grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD): U10 HD077680, U10 HD39005, U10 HD38992, U10 HD27049, U10 HD38998, U10 HD055942, HD055944, U10 HD055936 and U10 HD055925. This research was made possible by funding by the American Recovery and Reinvestment Act. Dr Hansen reports grants from NIH/NICHD and Yale University during the conduct of the study, grants from Roche Diagnostics and grants from Ferring International Pharmascience Center US outside the submitted work. Dr Peck reports support from Ferring Pharmaceuticals outside the submitted work. Dr Coward has nothing to disclose. Dr Wild reports grants from NICHD during the conduct of the study. Dr Trussell has nothing to disclose. Dr Krawetz reports grants from NICHD during the conduct of the study, grants from Merck and support from Taylor and Frances and from Springer, outside the submitted work. Dr Diamond reports grants from NIH/NICHD, Yale University, during the conduct of the study and support from Advanced Reproductive Care AbbVie, Bayer and ObsEva, outside the submitted work. Dr Legro reports support from Bayer, Kindex, Odega, Millendo and AbbVie and grants and support from Ferring, outside the submitted work. Dr Coutifaris reports grants from NICHD/NIH and personal fees from American Society for Reproductive Medicine, outside the submitted work. Dr Alvero has nothing to disclose. Dr Robinson reports grants from NIH during the conduct of the study. Dr Casson has nothing to disclose. Dr Christman reports grants from NICHD during the conduct of the study. Dr Santoro reports grants from NIH during the conduct of the study. Dr Zhang reports grants from NIH during the conduct of the study and support from Shangdong University outside the submitted work.
Trial registration number: n/a.
Keywords: intrauterine insemination; live birth; sperm total motile count; ultrasound guidance; unexplained infertility.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Effect of prematurely elevated late follicular progesterone on pregnancy outcomes following ovarian stimulation-intrauterine insemination for unexplained infertility: secondary analysis of the AMIGOS trial.Hum Reprod. 2024 Aug 1;39(8):1684-1691. doi: 10.1093/humrep/deae113. Hum Reprod. 2024. PMID: 38822675 Free PMC article. Clinical Trial.
-
Factors associated with study protocol adherence and bio banking participation in reproductive medicine clinical trials and their relationship to live birth.Hum Reprod. 2020 Dec 1;35(12):2819-2831. doi: 10.1093/humrep/deaa232. Hum Reprod. 2020. PMID: 33190149 Free PMC article. Clinical Trial.
-
Fertility-related quality of life from two RCT cohorts with infertility: unexplained infertility and polycystic ovary syndrome.Hum Reprod. 2016 Oct;31(10):2268-79. doi: 10.1093/humrep/dew175. Epub 2016 Jul 7. Hum Reprod. 2016. PMID: 27402910 Free PMC article. Clinical Trial.
-
Top 10 priorities for future infertility research: an international consensus development study.Fertil Steril. 2021 Jan;115(1):180-190. doi: 10.1016/j.fertnstert.2020.11.014. Epub 2020 Nov 30. Fertil Steril. 2021. PMID: 33272617
-
Agents for ovarian stimulation for intrauterine insemination (IUI) in ovulatory women with infertility.Cochrane Database Syst Rev. 2021 Nov 5;11(11):CD005356. doi: 10.1002/14651858.CD005356.pub3. Cochrane Database Syst Rev. 2021. PMID: 34739136 Free PMC article. Review.
Cited by
-
Predictive value of sperm motility before and after preparation for the pregnancy outcomes of intrauterine insemination.Clin Exp Reprod Med. 2021 Sep;48(3):255-261. doi: 10.5653/cerm.2021.04469. Epub 2021 Sep 1. Clin Exp Reprod Med. 2021. PMID: 34488289 Free PMC article.
-
Sperm Migration and Hyaluronic Acid Binding: Implications for Male Fertility Evaluation.Int J Mol Sci. 2024 Sep 17;25(18):9995. doi: 10.3390/ijms25189995. Int J Mol Sci. 2024. PMID: 39337482 Free PMC article.
-
Longitudinal semen parameter assessments and live birth: variability and implications for treatment strategies.Fertil Steril. 2022 Nov;118(5):852-863. doi: 10.1016/j.fertnstert.2022.08.012. Epub 2022 Oct 1. Fertil Steril. 2022. PMID: 36192231 Free PMC article. Clinical Trial.
-
Fertility Outcome and Safety of Ethiodized Poppy Seed Oil for Hysterosalpingography in 1,053 Infertile Patients: A Real-World Study.Front Med (Lausanne). 2022 Apr 15;9:804494. doi: 10.3389/fmed.2022.804494. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35492317 Free PMC article.
-
An Analysis of pre and post-Processing Semen Parameters at The Time of Intrauterine Insemination; and The Confounding Effects of Total Motile Sperm Counts on Pregnancy Outcome: A Prospective Cohort Study.Int J Fertil Steril. 2023 Nov 7;18(1):20-25. doi: 10.22074/ijfs.2023.560766.1355. Int J Fertil Steril. 2023. PMID: 38041455 Free PMC article.
References
-
- Alvero R, Hearns-Stokes RM, Catherino WH, Leondires MP, Segars JH. The presence of blood in the transfer catheter negatively influences outcome at embryo transfer. Hum Reprod 2003;18:1848–1852. - PubMed
-
- ASRM Practice Committee. Performing the embryo transfer: a guideline. Fertil Steril 2017;107:882–896. - PubMed
-
- Aydin Y, Hassa H, Oge T, Tokgoz VY. A randomized study of simultaneous hCG administration with intrauterine insemination in stimulated cycles. Eur J Obstet Gynecol Reprod Biol 2013;170:444–448. - PubMed
-
- Berker B, Kahraman K, Taskin S, Sukur YE, Sonmezer M, Atabekoglu CS. Recombinant FSH versus clomiphene citrate for ovarian stimulation in couples with unexplained infertility and male subfertility undergoing intrauterine insemination: a randomized trial. Arch Gynecol Obstet 2011;284:1561–1566. - PubMed
-
- Boomsma CM, Heineman MJ, Cohlen BJ, Farquhar C. Semen preparation techniques for intrauterine insemination. Cochrane Database Syst Rev 2007;Cd004507. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
