

Malignancy rates for Bethesda III and IV thyroid nodules: a retrospective study of the correlation between fine-needle aspiration cytology and histopathology
- PMID: 32293401
- PMCID: PMC7157988
- DOI: 10.1186/s12902-020-0530-9
Malignancy rates for Bethesda III and IV thyroid nodules: a retrospective study of the correlation between fine-needle aspiration cytology and histopathology
Abstract
Background: Fine-needle aspiration cytology (FNAC) has become a well-established modality in the diagnosis, staging and follow-up of thyroid nodules. FNAC outcomes are routinely classified using the Bethesda System for Reporting Thyroid Cytopathology (BSRTC), facilitating appropriate clinical management. Bethesda categories III and IV encompass varying risks of malignancy. This retrospective study established a possible association between these cytological categories and malignancy rates in patients treated at a single institution.
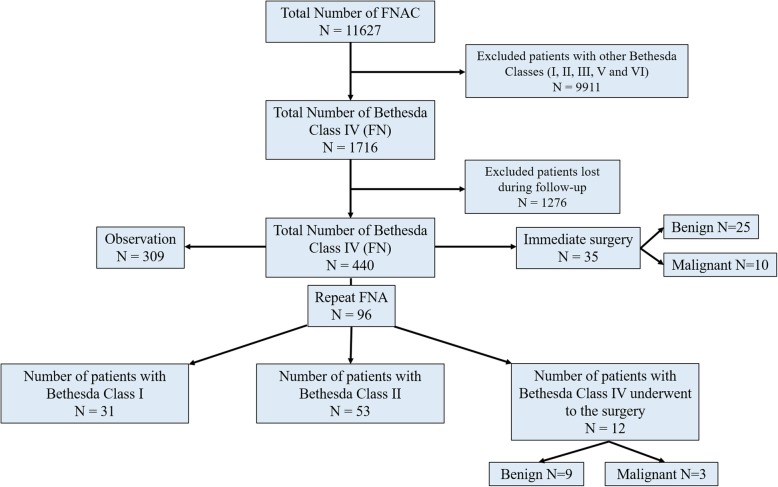
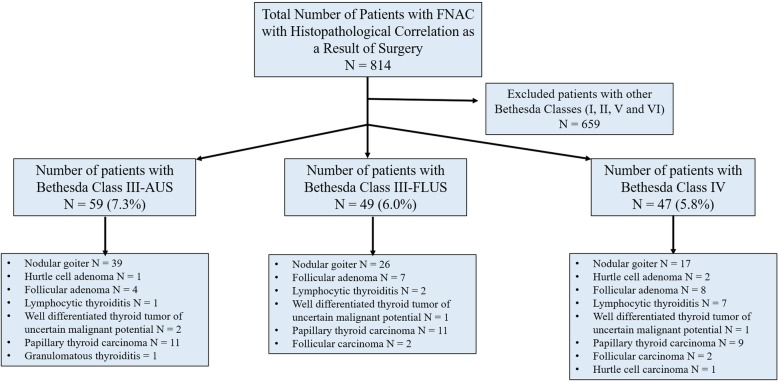
Methods: Over a 6-year period, 11,627 FNAC procedures were performed on thyroid nodules. Of these, 814 (59.63%) patients were submitted to thyroidectomy. The nodules of 108 patients were classified as Bethesda category III and 47 patients as Bethesda category IV. Patient data were reviewed to establish a correlation between the FNAC results and the final histopathological analyses.
Results: The rates of malignancy among patients who underwent surgery were 25% for category III and 27.6% for category IV, with no significant differences between categories (p = 0.67). The pathological parameters of malignant nodules, namely tumour type, size, encapsulation, invasion into the thyroid capsule, extrathyroidal extension and lymphovascular invasion did not significantly differ between the groups (p > 0.05).
Conclusions: This paper provides a more precise correlation of malignancy rates with thyroid nodules classified as Bethesda categories III and IV, as our findings are comparable to the literature, giving malignancy rates ranging from 10 to 30% for category III and 25-40% for category IV. Use of the BSRTC is heterogeneous across institutions, and there is some degree of subjectivity in the distinction between categories III and IV; therefore, it is crucial to estimate the rates of malignancy at each institution. Molecular assays are of increasing importance in determining the need for surgical intervention for thyroid lesions. Gene expression assays using FNAC material may demonstrate a high predictive value for cytologically indeterminate thyroid nodules diagnosed as Bethesda classes III and IV.
Keywords: Fine-needle aspiration cytology; Malignancy rate; Thyroid nodule; Thyroidectomy.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures

Similar articles
-
ACR TI-RADS and ATA US scores are helpful for the management of thyroid nodules with indeterminate cytology.BMC Endocr Disord. 2019 Oct 29;19(1):112. doi: 10.1186/s12902-019-0429-5. BMC Endocr Disord. 2019. PMID: 31664992 Free PMC article.
-
An innovative synthetic support for immunocytochemical assessment of cytologically indeterminate (Bethesda III) thyroid nodules.Front Endocrinol (Lausanne). 2022 Dec 1;13:1078019. doi: 10.3389/fendo.2022.1078019. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36531453 Free PMC article.
-
The Value of Ultrasound-Guided Fine-Needle Aspiration Cytology Combined with Puncture Feeling in the Diagnosis of Thyroid Nodules.Acta Cytol. 2021;65(5):368-376. doi: 10.1159/000517168. Epub 2021 Jul 16. Acta Cytol. 2021. PMID: 34350849
-
New perspectives in the diagnosis of thyroid follicular lesions.Int J Surg. 2017 May;41 Suppl 1:S7-S12. doi: 10.1016/j.ijsu.2017.03.020. Int J Surg. 2017. PMID: 28506417 Review.
-
Follow-up of atypia and follicular lesions of undetermined significance in thyroid fine needle aspiration cytology.Cytopathology. 2013 Dec;24(6):385-90. doi: 10.1111/cyt.12021. Epub 2012 Oct 18. Cytopathology. 2013. PMID: 23078633 Review.
Cited by
-
Clinical and ultrasonographic features in cancer risk stratification of indeterminate thyroid nodules.Saudi Med J. 2022 May;43(5):473-478. doi: 10.15537/smj.2022.43.5.20220045. Saudi Med J. 2022. PMID: 35537723 Free PMC article.
-
The Italian Consensus for the Classification and Reporting of Thyroid Cytology: Cytohistologic and molecular correlations on 37,371 nodules from a single institution.Cancer Cytopathol. 2022 Nov;130(11):899-912. doi: 10.1002/cncy.22618. Epub 2022 Jul 5. Cancer Cytopathol. 2022. PMID: 35789118 Free PMC article.
-
Impact of ultrasound elastography in evaluating Bethesda category IV thyroid nodules with histopathological correlation.Front Endocrinol (Lausanne). 2024 May 28;15:1393982. doi: 10.3389/fendo.2024.1393982. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38863927 Free PMC article.
-
The Accurate Interpretation and Clinical Significance of Morphological Features of Fine Needle Aspiration Cells in Papillary Thyroid Carcinoma.Anal Cell Pathol (Amst). 2023 May 3;2023:9397755. doi: 10.1155/2023/9397755. eCollection 2023. Anal Cell Pathol (Amst). 2023. PMID: 37181946 Free PMC article.
-
Gray zone Bethesda category III - Atypia of undetermined significance lesions of the thyroid: Potential diagnostic issues and image morphometry as a useful adjunct to cytomorphology.Cytojournal. 2024 Oct 17;21:38. doi: 10.25259/Cytojournal_86_2023. eCollection 2024. Cytojournal. 2024. PMID: 39563672 Free PMC article.
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid Cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid Cancer. Thyroid. 2016;26(1):1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
