

Meta-analysis on the use of hyaluronic acid gel to prevent intrauterine adhesion after intrauterine operations
- PMID: 32256748
- PMCID: PMC7086218
- DOI: 10.3892/etm.2020.8483
Meta-analysis on the use of hyaluronic acid gel to prevent intrauterine adhesion after intrauterine operations
Abstract
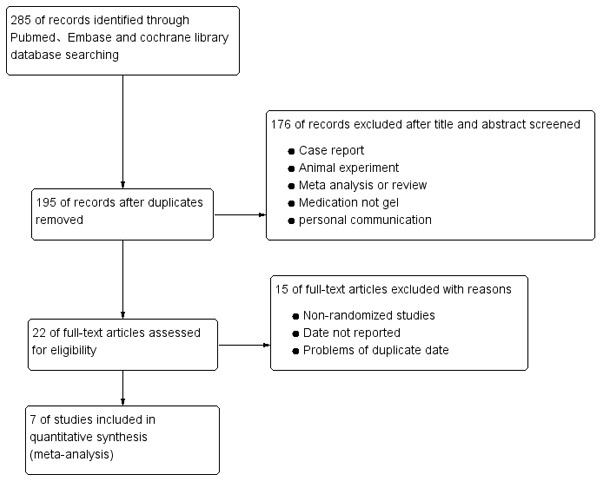
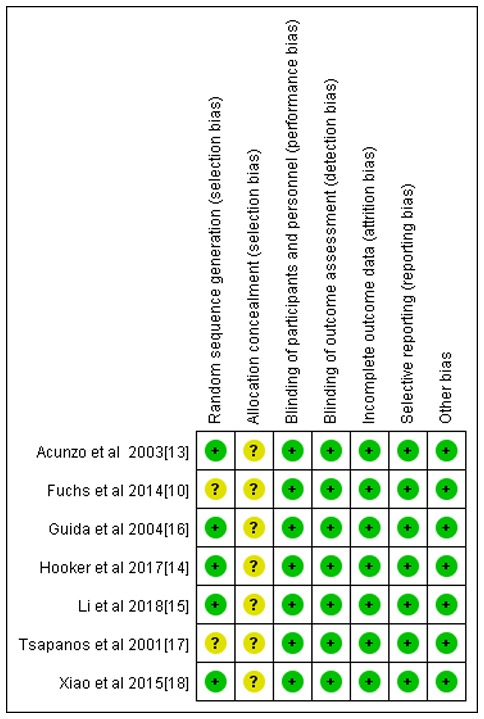
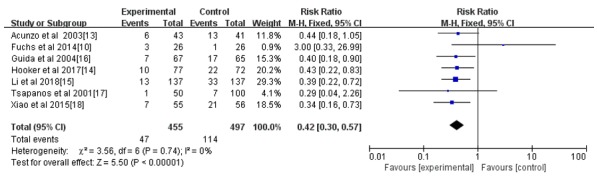
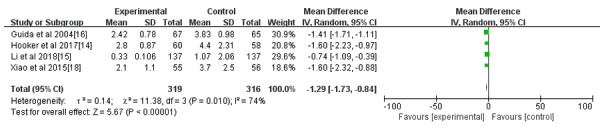
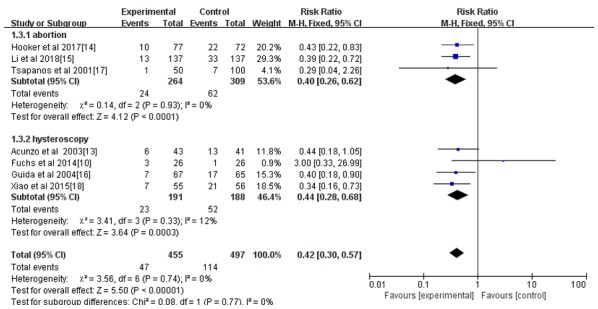
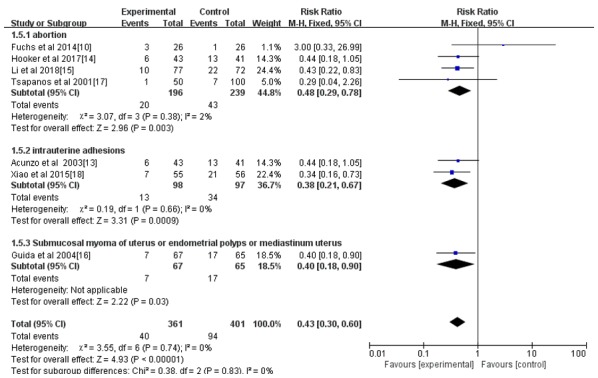
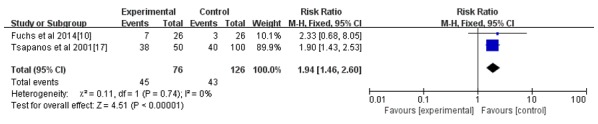
Intrauterine adhesion (IUA) is a severe complication that occurs following abortion, and hyaluronic acid gel has been used to prevent IUA following intrauterine operation. The present study aimed to systematically evaluate the efficacy of hyaluronic acid gel in preventing IUA following intrauterine operation. In the current study, a literature search was performed using PubMed, Cochrane Library and EMbase databases for randomized controlled clinical trials that used hyaluronic acid gel as an adjuvant therapy following intrauterine operation. The terms 'hyaluronic acid', 'intrauterine adhesions', 'Asherman's syndrome', 'IUA', 'dilatation and curettage', 'abortion' and 'hysteroscopic' were used to search for articles published online before July 31, 2018. RevMan 5.3 software was used to analyze the indicators of uterine cavity adhesion formation and pregnancy rates following intrauterine operation. A total of seven randomized controlled clinical studies were included, consisting of 952 patients who underwent intrauterine operation. The meta-analysis indicated that the use of hyaluronic acid gel reduced the incidence of IUA [relative risk (RR)=0.42; 95% confidence interval (CI)=0.30-0.57; P<0.001] and the score for IUA after an intrauterine operation (mean difference=-1.29; 95%=-1.73 to -0.84; P<0.001). A subgroup analysis revealed that the preventive effect of hyaluronic acid gel on IUA was not affected by the type of intrauterine operation, namely abortion (RR=0.40; 95% CI=0.26-0.62; P<0.001) and hysteroscopy (RR=0.44; 95% CI=0.28-0.68; P<0.001). The preventive effect of hyaluronic acid gel on IUA was also not affected by primary disorders/diseases including the following: Abortion (RR=0.48; 95% CI=0.29-0.78; P=0.003); IUA (RR=0.38; 95% CI=0.21-0.67; P<0.001) and submucosal myoma of the uterus, endometrial polyps or mediastinum uterus (RR=0.40; 95% CI=0.18-0.90; P=0.03). Hyaluronic acid gel improved pregnancy rates after intrauterine operations (RR=1.94; 95% CI=1.46-2.60; P<0.001). In conclusion, hyaluronic acid gel was indicated to significantly reduce the incidence of IUA following intrauterine operation, regardless of the type of intrauterine operation or the presence of primary diseases. Treatment with hyaluronic acid gel was also revealed to increase pregnancy rates following intrauterine operation.
Keywords: hyaluronic acid gel; intrauterine adhesions; intrauterine operation; pregnancy.
Copyright: © Zheng et al.
Figures
Similar articles
-
Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials.Life (Basel). 2020 Nov 15;10(11):285. doi: 10.3390/life10110285. Life (Basel). 2020. PMID: 33203159 Free PMC article.
-
Meta-analysis of the use of hyaluronic acid gel to prevent intrauterine adhesions after miscarriage.Eur J Obstet Gynecol Reprod Biol. 2020 Jan;244:1-4. doi: 10.1016/j.ejogrb.2019.10.018. Epub 2019 Oct 22. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 31731019 Review.
-
Meta-analysis on the use of hyaluronic acid gel to prevent recurrence of intrauterine adhesion after hysteroscopic adhesiolysis.Taiwan J Obstet Gynecol. 2019 Nov;58(6):731-736. doi: 10.1016/j.tjog.2019.09.002. Taiwan J Obstet Gynecol. 2019. PMID: 31759520 Review.
-
Short- and Long-term Outcomes of Postoperative Intrauterine Application of Hyaluronic Acid Gel: A Meta-analysis of Randomized Controlled Trials.J Minim Invasive Gynecol. 2022 Aug;29(8):934-942. doi: 10.1016/j.jmig.2022.05.006. Epub 2022 May 13. J Minim Invasive Gynecol. 2022. PMID: 35577245 Review.
-
Efficacy of hyaluronic acid on the prevention of intrauterine adhesion and the improvement of fertility: A meta-analysis of randomized trials.Complement Ther Clin Pract. 2022 May;47:101575. doi: 10.1016/j.ctcp.2022.101575. Epub 2022 Mar 23. Complement Ther Clin Pract. 2022. PMID: 35349823 Review.
Cited by
-
Crosslinked Hyaluronic Acid Gels for the Prevention of Intrauterine Adhesions after a Hysteroscopic Myomectomy in Women with Submucosal Myomas: A Prospective, Randomized, Controlled Trial.Life (Basel). 2020 May 15;10(5):67. doi: 10.3390/life10050067. Life (Basel). 2020. PMID: 32429137 Free PMC article.
-
VitroGel-loaded human MenSCs promote endometrial regeneration and fertility restoration.Front Bioeng Biotechnol. 2024 Jan 8;11:1310149. doi: 10.3389/fbioe.2023.1310149. eCollection 2023. Front Bioeng Biotechnol. 2024. PMID: 38260736 Free PMC article.
-
Efficacy of Applying Hyaluronic Acid Gels in the Primary Prevention of Intrauterine Adhesion after Hysteroscopic Myomectomy: A Meta-Analysis of Randomized Controlled Trials.Life (Basel). 2020 Nov 15;10(11):285. doi: 10.3390/life10110285. Life (Basel). 2020. PMID: 33203159 Free PMC article.
-
Recent developments in bio-scaffold materials as delivery strategies for therapeutics for endometrium regeneration.Mater Today Bio. 2021 Feb 25;11:100101. doi: 10.1016/j.mtbio.2021.100101. eCollection 2021 Jun. Mater Today Bio. 2021. PMID: 34036261 Free PMC article. Review.
-
HYSTEROSCOPIC MYOMECTOMY.Medicina (Kaunas). 2022 Nov 11;58(11):1627. doi: 10.3390/medicina58111627. Medicina (Kaunas). 2022. PMID: 36422166 Free PMC article. Review.
References
-
- Vancaillie TG, Garad R. Asherman's syndrome. Aust Nurs J. 2013;20:34–36. - PubMed
-
- Mehedintu C, Ionescu O, Rotaru AM, Antonovici M, Plotogea M, Berceanu C, Vladareanu S, Bratila E. Asherman's syndrome after an uncomplicated cesarian section. Gineco. 2016;12:166–168.
LinkOut - more resources
Full Text Sources