

Intratumoral Immunotherapy-Update 2019
- PMID: 32162802
- PMCID: PMC7066689
- DOI: 10.1634/theoncologist.2019-0438
Intratumoral Immunotherapy-Update 2019
Abstract
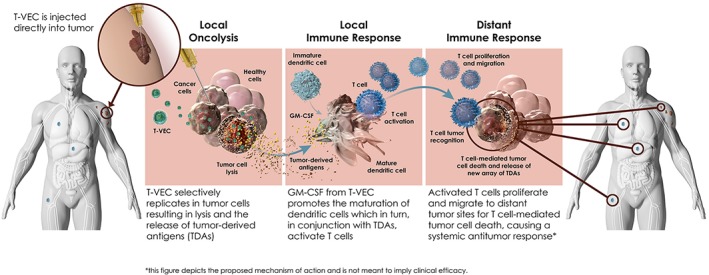
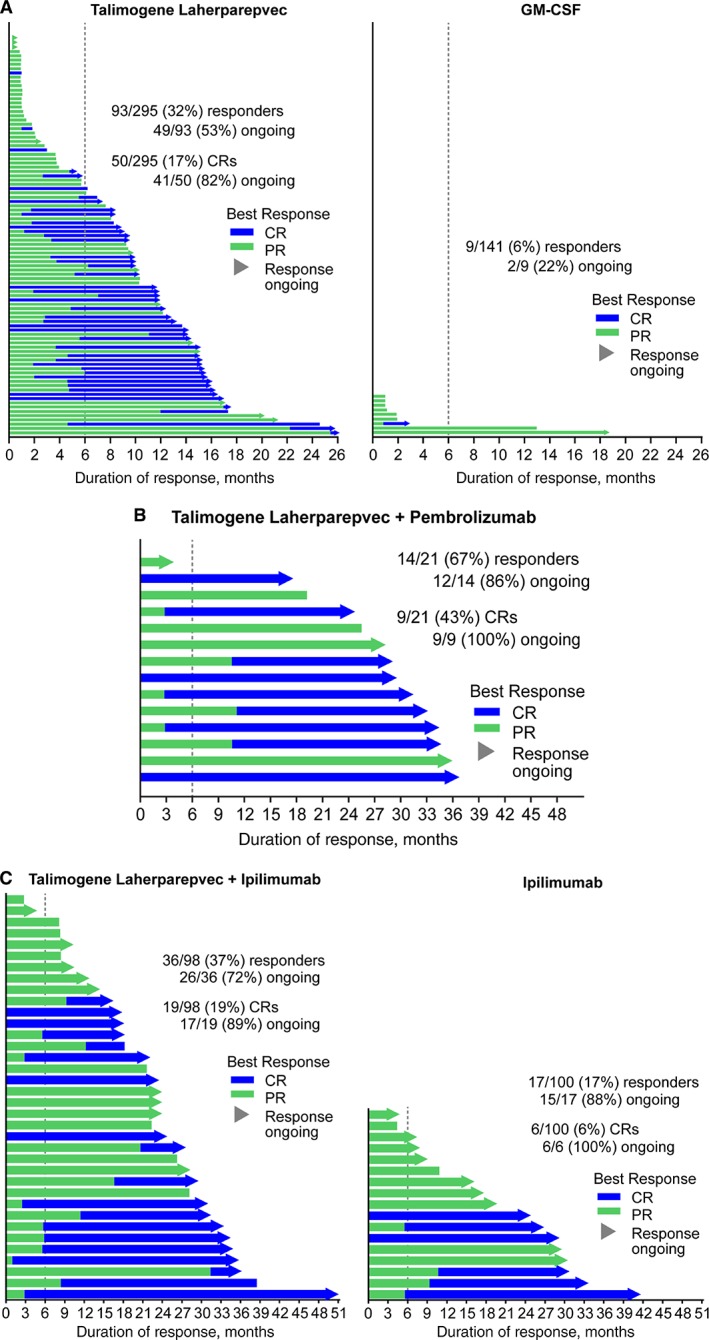
Intratumoral immunotherapies aim to trigger local and systemic immunologic responses via direct injection of immunostimulatory agents with the goal of tumor cell lysis, followed by release of tumor-derived antigens and subsequent activation of tumor-specific effector T cells. In 2019, a multitude of intratumoral immunotherapies with varied mechanisms of action, including nononcolytic viral therapies such as PV-10 and toll-like receptor 9 agonists and oncolytic viral therapies such as CAVATAK, Pexa-Vec, and HF10, have been extensively evaluated in clinical trials and demonstrated promising antitumor activity with tolerable toxicities in melanoma and other solid tumor types. Talimogene laherparepvec (T-VEC), a genetically modified herpes simplex virus type 1-based oncolytic immunotherapy, is the first oncolytic virus approved by the U.S. Food and Drug Administration for the treatment of unresectable melanoma recurrent after initial surgery. In patients with unresectable metastatic melanoma, T-VEC demonstrated a superior durable response rate (continuous complete response or partial response lasting ≥6 months) over subcutaneous GM-CSF (16.3% vs. 2.1%; p < .001). Responses were seen in both injected and uninjected lesions including visceral lesions, suggesting a systemic antitumor response. When combined with immune checkpoint inhibitors, T-VEC significantly improved response rates compared with single agent; similar results were seen with combinations of checkpoint inhibitors and other intratumoral therapies such as CAVATAK, HF10, and TLR9 agonists. In this review, we highlight recent results from clinical trials of key intratumoral immunotherapies that are being evaluated in the clinic, with a focus on T-VEC in the treatment of advanced melanoma as a model for future solid tumor indications. IMPLICATIONS FOR PRACTICE: This review provides oncologists with the latest information on the development of key intratumoral immunotherapies, particularly oncolytic viruses. Currently, T-VEC is the only U.S. Food and Drug Administration (FDA)-approved oncolytic immunotherapy. This article highlights the efficacy and safety data from clinical trials of T-VEC both as monotherapy and in combination with immune checkpoint inhibitors. This review summarizes current knowledge on intratumoral therapies, a novel modality with increased utility in cancer treatment, and T-VEC, the only U.S. FDA-approved oncolytic viral therapy, for medical oncologists. This review evaluates approaches to incorporate T-VEC into daily practice to offer the possibility of response in selected melanoma patients with manageable adverse events as compared with other available immunotherapies.
Keywords: Immune checkpoint inhibitors; Intratumoral immunotherapies; Melanoma; OPTiM; Talimogene laherparepvec.
© 2019 The Authors. The Oncologist published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Conflict of interest statement
Figures

Similar articles
-
Talimogene Laherparepvec: An Oncolytic Virus Therapy for Melanoma.Ann Pharmacother. 2017 Aug;51(8):675-681. doi: 10.1177/1060028017702654. Epub 2017 Mar 28. Ann Pharmacother. 2017. PMID: 28351167 Review.
-
Clinical development of talimogene laherparepvec (T-VEC): a modified herpes simplex virus type-1-derived oncolytic immunotherapy.Expert Rev Anticancer Ther. 2015;15(12):1389-403. doi: 10.1586/14737140.2015.1115725. Expert Rev Anticancer Ther. 2015. PMID: 26558498 Review.
-
Engineered oncolytic viruses to treat melanoma: where are we now and what comes next?Expert Opin Biol Ther. 2018 Dec;18(12):1199-1207. doi: 10.1080/14712598.2018.1544614. Expert Opin Biol Ther. 2018. PMID: 30392405 Review.
-
Talimogene Laherparepvec (T-VEC): An Intralesional Cancer Immunotherapy for Advanced Melanoma.Cancers (Basel). 2021 Mar 18;13(6):1383. doi: 10.3390/cancers13061383. Cancers (Basel). 2021. PMID: 33803762 Free PMC article. Review.
-
The safety of talimogene laherparepvec for the treatment of advanced melanoma.Expert Opin Drug Saf. 2017 Feb;16(2):265-269. doi: 10.1080/14740338.2017.1274729. Epub 2016 Dec 28. Expert Opin Drug Saf. 2017. PMID: 27989216 Review.
Cited by
-
Encapsulation of miRNA and siRNA into Nanomaterials for Cancer Therapeutics.Pharmaceutics. 2022 Aug 3;14(8):1620. doi: 10.3390/pharmaceutics14081620. Pharmaceutics. 2022. PMID: 36015246 Free PMC article. Review.
-
Revisiting targeted therapy and immunotherapy for advanced cholangiocarcinoma.Front Immunol. 2023 Mar 1;14:1142690. doi: 10.3389/fimmu.2023.1142690. eCollection 2023. Front Immunol. 2023. PMID: 36936931 Free PMC article. Review.
-
Beyond Immunotherapy: Seizing the Momentum of Oncolytic Viruses in the Ideal Platform of Skin Cancers.Cancers (Basel). 2022 Jun 10;14(12):2873. doi: 10.3390/cancers14122873. Cancers (Basel). 2022. PMID: 35740539 Free PMC article. Review.
-
Latest evidence on immunotherapy for cholangiocarcinoma.Oncol Lett. 2020 Dec;20(6):381. doi: 10.3892/ol.2020.12244. Epub 2020 Oct 23. Oncol Lett. 2020. PMID: 33154779 Free PMC article. Review.
-
Prospects of Synergy: Local Interventions and CAR T Cell Therapy in Solid Tumors.BioDrugs. 2024 Sep;38(5):611-637. doi: 10.1007/s40259-024-00669-y. Epub 2024 Jul 30. BioDrugs. 2024. PMID: 39080180 Free PMC article. Review.
References
-
- Schuster M, Nechansky A, Kircheis R. Cancer immunotherapy. Biotechnol J 2006;1:138–147. - PubMed
-
- Vesely MD, Kershaw MH, Schreiber RD et al. Natural innate and adaptive immunity to cancer. Ann Rev Immunol 2011;29:235–271. - PubMed
-
- Waldhauer I, Steinle A. NK cells and cancer immunosurveillance. Oncogene 2008;27:5932–5943. - PubMed
-
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: Integrating immunity's roles in cancer suppression and promotion. Science 2011;331:1565–1570. - PubMed
-
- Coley WB. The treatment of malignant tumors by repeated inoculations of erysipelas. With a report of ten original cases. 1893. Am J Med Sci 1893;105:487–510. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
