

The relationship between environmental sources and the susceptibility of Acanthamoeba keratitis in the United Kingdom
- PMID: 32160218
- PMCID: PMC7065798
- DOI: 10.1371/journal.pone.0229681
The relationship between environmental sources and the susceptibility of Acanthamoeba keratitis in the United Kingdom
Abstract
Purpose: To determine whether Acanthamoeba keratitis (AK) patients have higher rates of Acanthamoeba and free-living amoeba (FLA) colonising domestic sinks than control contact lens (CL) wearers, and whether these isolates are genetically similar to the corneal isolates from their CL associated AK.
Methods: 129 AK patients from Moorefield Eye Hospital, London and 64 control CL wearers from the Institute of Optometry were included in this study. The participants self-collected home kitchen and bathroom samples from tap-spouts, overflows and drains using an instructional kit. The samples were cultured by inoculating onto a non-nutrient agar plate seeded with Escherichia coli, incubated at 32°C and examined for amoebae by microscopy for up to 2 weeks. Partial sequences of mitochondrial cytochrome oxidase genes (coxA) of Acanthamoeba isolates from four AK patients were compared to Acanthamoeba isolated from the patient's home. The association between sampling sites was analysed with the chi-square test.
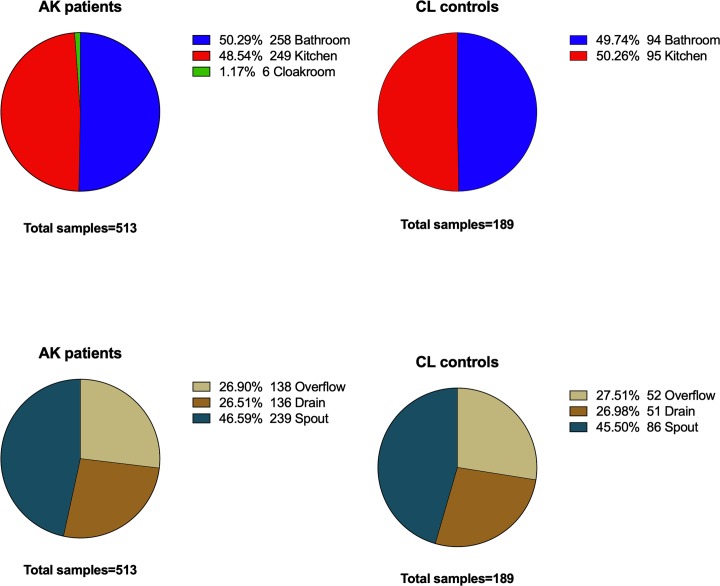
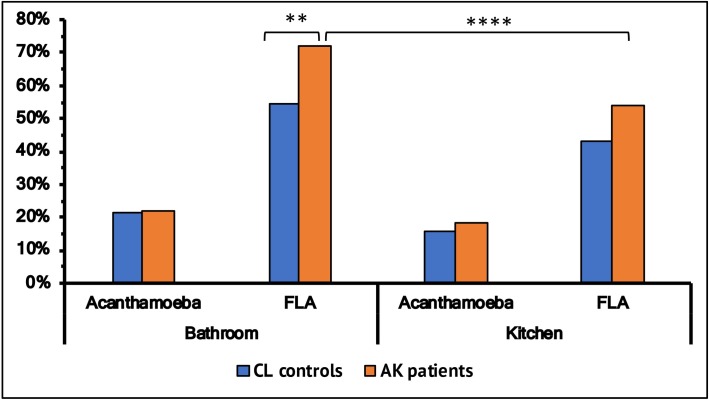
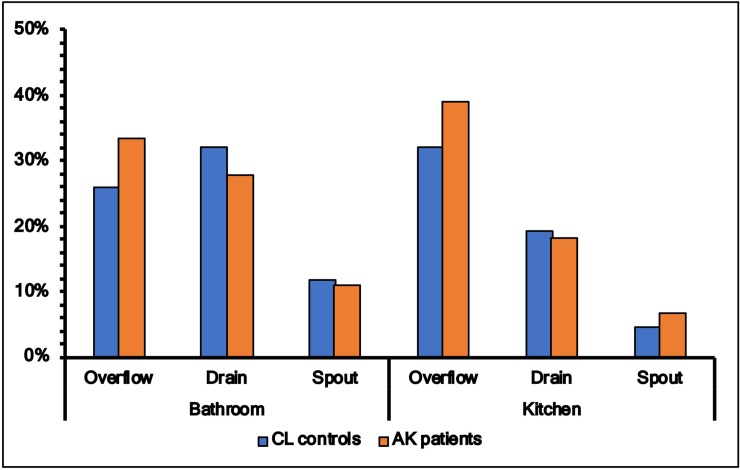
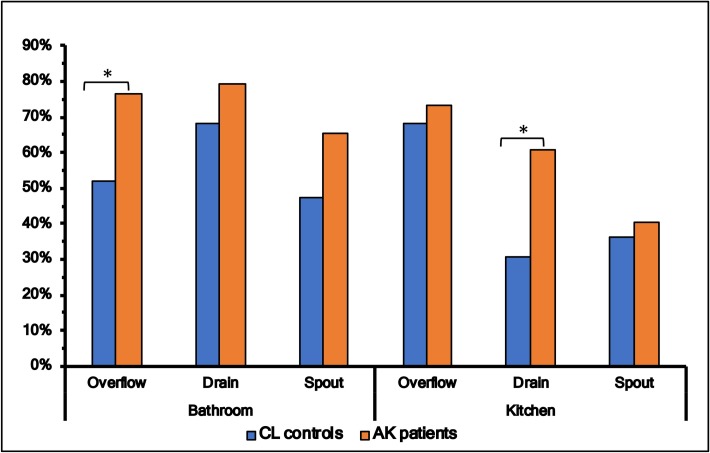
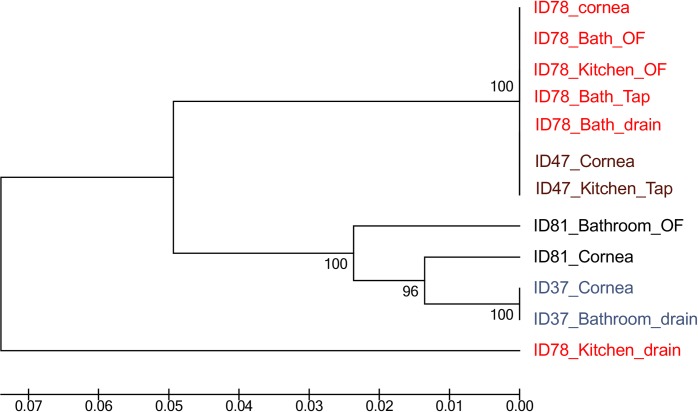
Results: A total of 513 samples from AK patients and 189 from CL controls were collected. The yield of FLA was significantly greater in patients' bathrooms (72.1%) than CL controls' bathrooms (53.4%) (p<0.05). Spouts (kitchen 6.7%, bathroom 11%) had the lowest rate of Acanthamoeba isolation compared to drains (kitchen 18.2%, bathroom 27.9%) and overflow (kitchen 39.1%, bathroom 25.9%) either in kitchens or bathrooms (p<0.05). There was no statistically significant difference between the average prevalence of Acanthamoeba in all three sample sites in kitchens (16.9%) compared to all three sample sites in bathrooms (21.5%) and no association for Acanthamoeba prevalence between AK patients and CL controls. All four corneal isolates had the same coxA sequence as at least one domestic water isolate from the patients' sink of the kitchen and the bathroom.
Conclusion: The prevalence of Acanthamoeba and FLA was high in UK homes. FLA colonisation was higher in AK patients compared to controls but the prevalence of Acanthamoeba between AK patients and CL controls domestic sinks was similar. This study confirms that domestic water isolates are probably the source of AK infection. Advice about avoiding water contact when using CL's should be mandatory.
Conflict of interest statement
SC is employed by Research Organisation (KC) Ltd. SK is employed by Ophtecs Corporation. There are no patents, products in development, or marketed products to declare. The commercial affiliation does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Acanthamoeba keratitis: the role of domestic tap water contamination in the United Kingdom.Invest Ophthalmol Vis Sci. 2004 Jan;45(1):165-9. doi: 10.1167/iovs.03-0559. Invest Ophthalmol Vis Sci. 2004. PMID: 14691169
-
The role of domestic tap water on Acanthamoeba keratitis in non-contact lens wearers and validation of laboratory methods.Parasitol Res. 2015 Sep;114(9):3283-9. doi: 10.1007/s00436-015-4549-1. Epub 2015 May 29. Parasitol Res. 2015. PMID: 26017346
-
Acanthamoeba keratitis in noncompliant soft contact lenses users: Genotyping and risk factors, a study from Cairo, Egypt.J Infect Public Health. 2018 May-Jun;11(3):377-383. doi: 10.1016/j.jiph.2017.09.013. Epub 2017 Sep 28. J Infect Public Health. 2018. PMID: 28965795
-
Acanthamoeba keratitis: an emerging disease gathering importance worldwide?Trends Parasitol. 2013 Apr;29(4):181-7. doi: 10.1016/j.pt.2013.01.006. Epub 2013 Feb 21. Trends Parasitol. 2013. PMID: 23433689 Review.
-
Acanthamoeba: a review of its potential to cause keratitis, current lens care solution disinfection standards and methodologies, and strategies to reduce patient risk.Eye Contact Lens. 2008 Sep;34(5):247-53. doi: 10.1097/ICL.0b013e31817e7d83. Eye Contact Lens. 2008. PMID: 18779663 Review.
Cited by
-
A history of over 40 years of potentially pathogenic free-living amoeba studies in Brazil - a systematic review.Mem Inst Oswaldo Cruz. 2022 Jul 1;117:e210373. doi: 10.1590/0074-02760210373. eCollection 2022. Mem Inst Oswaldo Cruz. 2022. PMID: 35792751 Free PMC article.
-
American Academy of Optometry Microbial Keratitis Think Tank.Optom Vis Sci. 2021 Mar 1;98(3):182-198. doi: 10.1097/OPX.0000000000001664. Optom Vis Sci. 2021. PMID: 33771951 Free PMC article.
-
Acanthamoeba keratitis: Molecular typing of Acanthamoeba species directly from ocular tissue.Curr Res Parasitol Vector Borne Dis. 2023 Aug 23;4:100141. doi: 10.1016/j.crpvbd.2023.100141. eCollection 2023. Curr Res Parasitol Vector Borne Dis. 2023. PMID: 37680763 Free PMC article.
-
Assessment of genotypes, endosymbionts and clinical characteristics of Acanthamoeba recovered from ocular infection.BMC Infect Dis. 2022 Sep 29;22(1):757. doi: 10.1186/s12879-022-07741-4. BMC Infect Dis. 2022. PMID: 36175838 Free PMC article.
-
A simple method for culturing Acanthamoeba from soft contact lens at a clinical laboratory of a hospital: Case report of Acanthamoeba keratitis.Clin Case Rep. 2023 Nov 20;11(11):e8248. doi: 10.1002/ccr3.8248. eCollection 2023 Nov. Clin Case Rep. 2023. PMID: 38028087 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
