

Choice of Study Populations for Vaccines
- PMID: 32134487
- PMCID: PMC7057788
- DOI: 10.1093/infdis/jiz537
Choice of Study Populations for Vaccines
Abstract
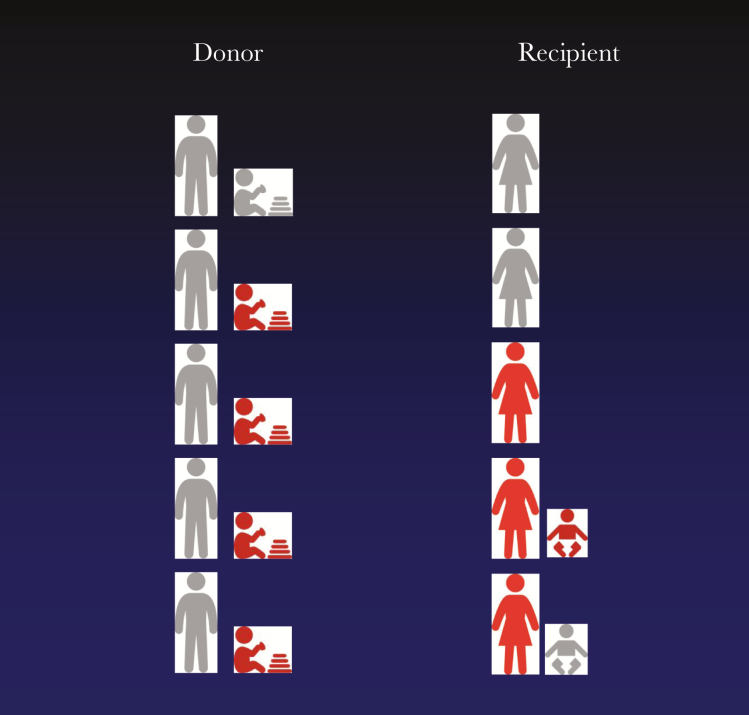
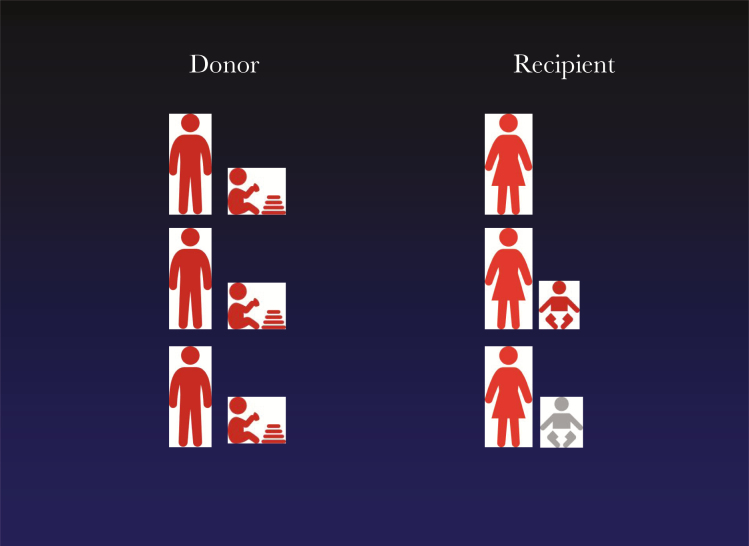
The natural history of cytomegalovirus (CMV) infection is complex. Individuals may experience primary infection, reactivation of latent infection, or reinfection with a new strain despite natural immunity. The ability of this virus to continue to replicate despite substantial immune responses is attributable to the many immune evasion genes encoded within its genome. Given this complex natural history and immunology, the design of clinical trials of CMV vaccines may require components not usually found in trials of vaccines designed to protect against viruses that cause only acute infections. In this article, we focus on specific aspects of clinical trial design that could be adopted to address the complexities of CMV infections. We consider women of childbearing age, toddlers, recipients of solid organ transplantation, and stem cell transplant patients, emphasizing the parallels between women and solid organ transplantation that could allow vaccines to be developed in parallel in both these patient groups. We emphasize the potential for studies of passive immunity to inform the selection of immunogens as candidates for active immunization and vice versa. We also illustrate how application of whole-genomic sequencing could document whether vaccines protect against reactivation or reinfection of CMV or both.
Keywords: ante-natal; cytomegalovirus; immune responses; transplant; vaccination.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Scientific and Regulatory Considerations for Efficacy Studies of Cytomegalovirus Vaccines.J Infect Dis. 2020 Mar 5;221(Suppl 1):S103-S108. doi: 10.1093/infdis/jiz523. J Infect Dis. 2020. PMID: 32134485 Review.
-
Vaccination against the human cytomegalovirus.Vaccine. 2019 Nov 28;37(50):7437-7442. doi: 10.1016/j.vaccine.2018.02.089. Epub 2018 Apr 3. Vaccine. 2019. PMID: 29622379 Free PMC article. Review.
-
The Status of Vaccine Development Against the Human Cytomegalovirus.J Infect Dis. 2020 Mar 5;221(Suppl 1):S113-S122. doi: 10.1093/infdis/jiz447. J Infect Dis. 2020. PMID: 32134478 Free PMC article. Review.
-
Criteria to define interruption of transmission of human cytomegalovirus from organ donor to recipient.Rev Med Virol. 2018 Jan;28(1). doi: 10.1002/rmv.1958. Epub 2017 Nov 17. Rev Med Virol. 2018. PMID: 29148608 Review.
-
Preventing Infection by Human Cytomegalovirus.J Infect Dis. 2020 Mar 5;221(Suppl 1):S123-S127. doi: 10.1093/infdis/jiz448. J Infect Dis. 2020. PMID: 32134484 Free PMC article. Review.
Cited by
-
Seroprevalence of Cytomegalovirus and Associated Factors Among Preconception Women: A Cross-Sectional Nationwide Study in China.Front Public Health. 2021 Aug 25;9:631411. doi: 10.3389/fpubh.2021.631411. eCollection 2021. Front Public Health. 2021. PMID: 34513776 Free PMC article.
-
Pathogenesis of human cytomegalovirus in the immunocompromised host.Nat Rev Microbiol. 2021 Dec;19(12):759-773. doi: 10.1038/s41579-021-00582-z. Epub 2021 Jun 24. Nat Rev Microbiol. 2021. PMID: 34168328 Free PMC article. Review.
References
-
- Cope AV, Sabin C, Burroughs A, Rolles K, Griffiths PD, Emery VC. Interrelationships among quantity of human cytomegalovirus (HCMV) DNA in blood, donor-recipient serostatus, and administration of methylprednisolone as risk factors for HCMV disease following liver transplantation. J Infect Dis 1997; 176:1484–90. - PubMed
-
- Paya C, Humar A, Dominguez E, et al. ; Valganciclovir Solid Organ Transplant Study Group Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant 2004; 4:611–20. - PubMed
-
- Humar A, Lebranchu Y, Vincenti F, et al. . The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients. Am J Transplant 2010; 10:1228–37. - PubMed
-
- Singh N. Antiviral drugs for cytomegalovirus in transplant recipients: advantages of preemptive therapy. Rev Med Virol 2006; 16:281–7. - PubMed
