

Immunotherapy with immune checkpoint inhibitors in colorectal cancer: what is the future beyond deficient mismatch-repair tumours?
- PMID: 32104582
- PMCID: PMC7034232
- DOI: 10.1093/gastro/goz061
Immunotherapy with immune checkpoint inhibitors in colorectal cancer: what is the future beyond deficient mismatch-repair tumours?
Abstract
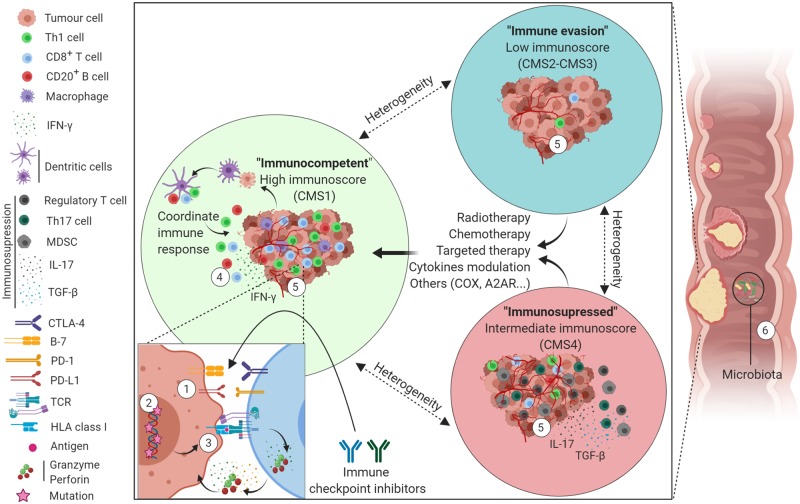
Following initial success in melanoma and lung tumours, immune checkpoint inhibitors (ICIs) are now well recognized as a major immunotherapy treatment modality for multiple types of solid cancers. In colorectal cancer (CRC), the small subset that is mismatch-repair-deficient and microsatellite-instability-high (dMMR/MSI-H) derive benefit from immunotherapy; however, the vast majority of patients with proficient MMR (pMMR) or with microsatellite stable (MSS) CRC do not. Immunoscore and the consensus molecular subtype classifications are promising biomarkers in predicting therapeutic efficacy in selected CRC. In pMRR/MSS CRC, biomarkers are also needed to understand the molecular mechanisms governing immune reactivity and to predict their relationship to treatment. The continuous development of such biomarkers would offer new perspectives and more personalized treatments by targeting oncological options, including ICIs, which modify the tumour-immune microenvironment. In this review, we focus on CRC and discuss the current status of ICIs, the role of biomarkers to predict response to immunotherapy, and the approaches being explored to render pMMR/MSS CRC more immunogenic through the use of combined therapies.
Keywords: colorectal cancer; immune checkpoint inhibitors; immune response; immunoscore; immunotherapy.
© The Author(s) 2019. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Figures
Similar articles
-
Biomarkers of Response and Resistance to Immunotherapy in Microsatellite Stable Colorectal Cancer: Toward a New Personalized Medicine.Cancers (Basel). 2022 Apr 29;14(9):2241. doi: 10.3390/cancers14092241. Cancers (Basel). 2022. PMID: 35565369 Free PMC article. Review.
-
Immunotherapy efficacy on mismatch repair-deficient colorectal cancer: From bench to bedside.Biochim Biophys Acta Rev Cancer. 2020 Dec;1874(2):188447. doi: 10.1016/j.bbcan.2020.188447. Epub 2020 Oct 6. Biochim Biophys Acta Rev Cancer. 2020. PMID: 33035640 Free PMC article. Review.
-
Regorafenib in combination with immune checkpoint inhibitors for mismatch repair proficient (pMMR)/microsatellite stable (MSS) colorectal cancer.Cancer Treat Rev. 2022 Nov;110:102460. doi: 10.1016/j.ctrv.2022.102460. Epub 2022 Aug 27. Cancer Treat Rev. 2022. PMID: 36058142 Review.
-
Application of immune checkpoint inhibitors in colorectal cancer.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021 Aug 28;46(8):894-899. doi: 10.11817/j.issn.1672-7347.2021.200872. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 34565736 Free PMC article. Chinese, English.
-
The next bastion to be conquered in immunotherapy: microsatellite stable colorectal cancer.Front Immunol. 2023 Dec 22;14:1298524. doi: 10.3389/fimmu.2023.1298524. eCollection 2023. Front Immunol. 2023. PMID: 38187388 Free PMC article. Review.
Cited by
-
Immunomodulation by Inflammation during Liver and Gastrointestinal Tumorigenesis and Aging.Int J Mol Sci. 2021 Feb 24;22(5):2238. doi: 10.3390/ijms22052238. Int J Mol Sci. 2021. PMID: 33668122 Free PMC article. Review.
-
A dynamic CD2-rich compartment at the outer edge of the immunological synapse boosts and integrates signals.Nat Immunol. 2020 Oct;21(10):1232-1243. doi: 10.1038/s41590-020-0770-x. Epub 2020 Sep 14. Nat Immunol. 2020. PMID: 32929275 Free PMC article.
-
T cell factor 1 (TCF-1) defines T cell differentiation in colorectal cancer.iScience. 2024 Aug 22;27(9):110754. doi: 10.1016/j.isci.2024.110754. eCollection 2024 Sep 20. iScience. 2024. PMID: 39280606 Free PMC article.
-
"Cold" colorectal cancer faces a bottleneck in immunotherapy.World J Gastrointest Oncol. 2023 Feb 15;15(2):240-250. doi: 10.4251/wjgo.v15.i2.240. World J Gastrointest Oncol. 2023. PMID: 36908324 Free PMC article. Review.
-
The role of immunogenic cell death in gastrointestinal cancer immunotherapy (Review).Biomed Rep. 2021 Oct;15(4):86. doi: 10.3892/br.2021.1462. Epub 2021 Aug 17. Biomed Rep. 2021. PMID: 34512974 Free PMC article. Review.
References
-
- Ferlay J, Colombet M, Soerjomataram I. et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 2019;144:1941–53. - PubMed
-
- Arnold M, Sierra MS, Laversanne M. et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017;66:683–91. - PubMed
-
- Schreiber RD, Old LJ, Smyth MJ.. Cancer immunoediting: integrating immunity's roles in cancer suppression and promotion. Science 2011;331:1565–70. - PubMed
-
- Sharma P, Allison JP.. The future of immune checkpoint therapy. Science 2015;348:56–61. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
