

The effect of 90-90-90 on HIV-1 incidence and mortality in eSwatini: a mathematical modelling study
- PMID: 32061317
- PMCID: PMC7221345
- DOI: 10.1016/S2352-3018(19)30436-9
The effect of 90-90-90 on HIV-1 incidence and mortality in eSwatini: a mathematical modelling study
Abstract
Background: The rapid scale-up of antiretroviral therapy (ART) towards the UNAIDS 90-90-90 goals over the last decade has sparked considerable debate as to whether universal test and treat can end the HIV-1 epidemic in sub-Saharan Africa. We aimed to develop a network transmission model, calibrated to capture age-specific and sex-specific gaps in the scale-up of ART, to estimate the historical and future effect of attaining and surpassing the UNAIDS 90-90-90 treatment targets on HIV-1 incidence and mortality, and to assess whether these interventions will be enough to achieve epidemic control (incidence of 1 infection per 1000 person-years) by 2030.
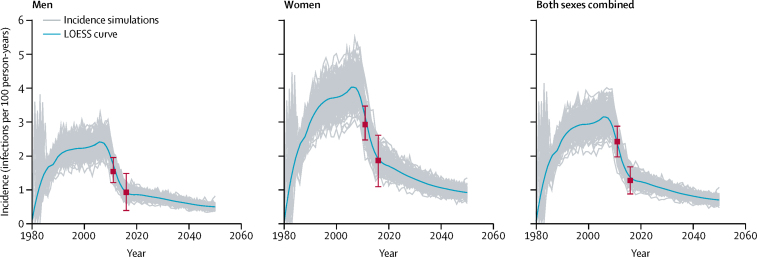
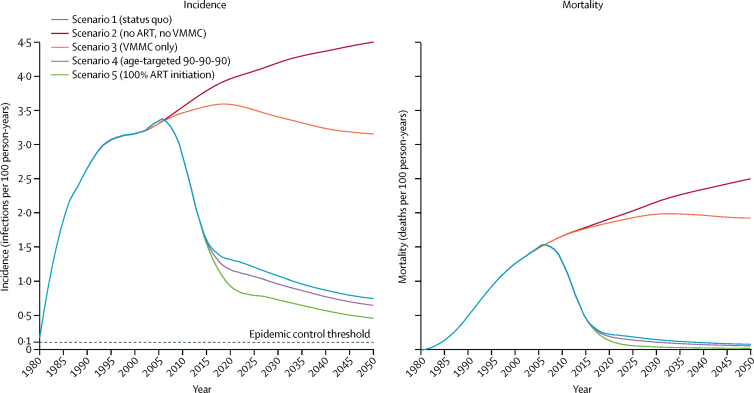
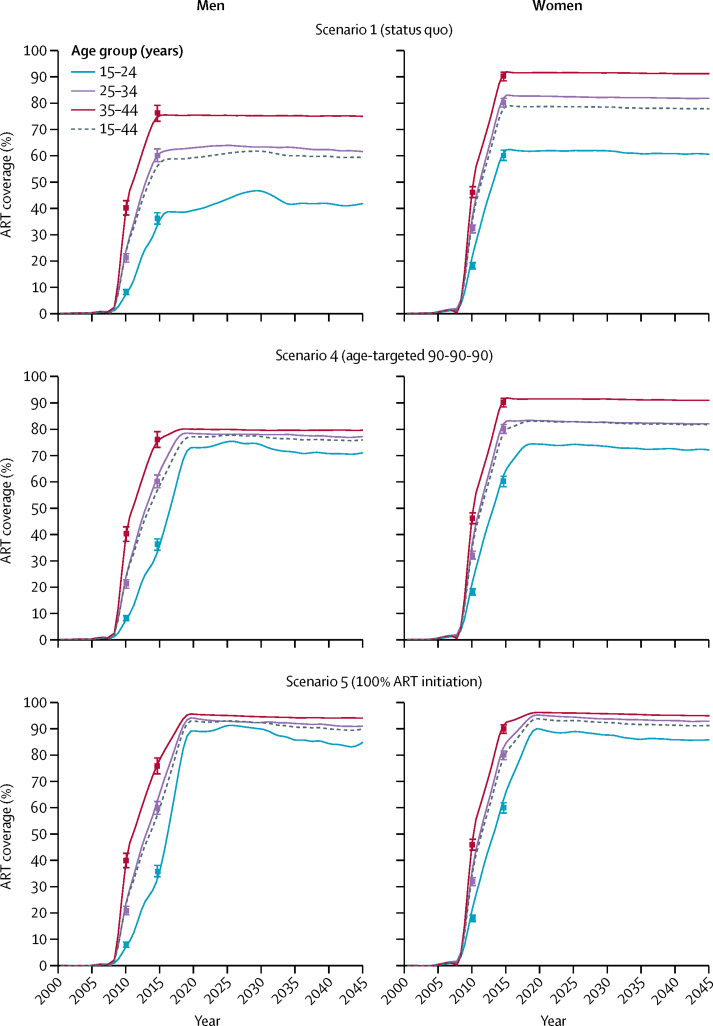
Methods: We used eSwatini (formerly Swaziland) as a case study to develop our model. We used data on HIV prevalence by 5-year age bins, sex, and year from the 2007 Swaziland Demographic Health Survey (SDHS), the 2011 Swaziland HIV Incidence Measurement Survey, and the 2016 Swaziland Population Health Impact Assessment (PHIA) survey. We estimated the point prevalence of ART coverage among all HIV-infected individuals by age, sex, and year. Age-specific data on the prevalence of male circumcision from the SDHS and PHIA surveys were used as model inputs for traditional male circumcision and scale-up of voluntary medical male circumcision (VMMC). We calibrated our model using publicly available data on demographics; HIV prevalence by 5-year age bins, sex, and year; and ART coverage by age, sex, and year. We modelled the effects of five scenarios (historical scale-up of ART and VMMC [status quo], no ART or VMMC, no ART, age-targeted 90-90-90, and 100% ART initiation) to quantify the contribution of ART scale-up to declines in HIV incidence and mortality in individuals aged 15-49 by 2016, 2030, and 2050.
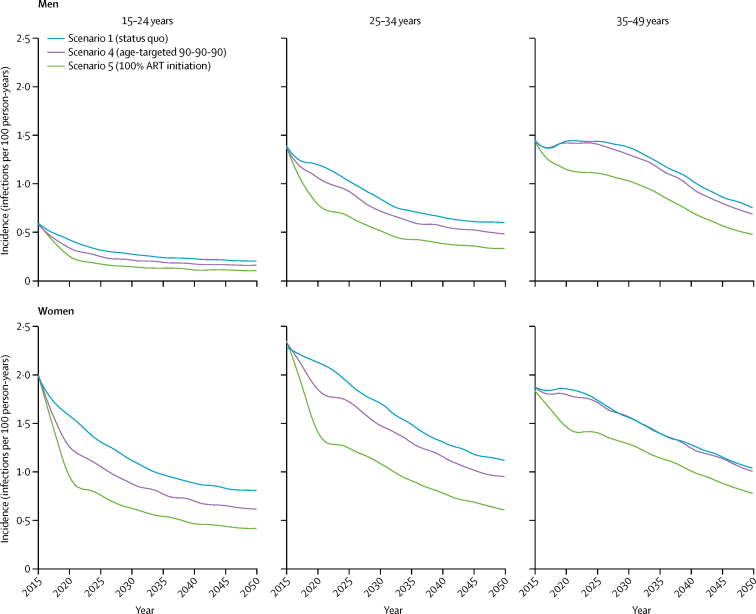
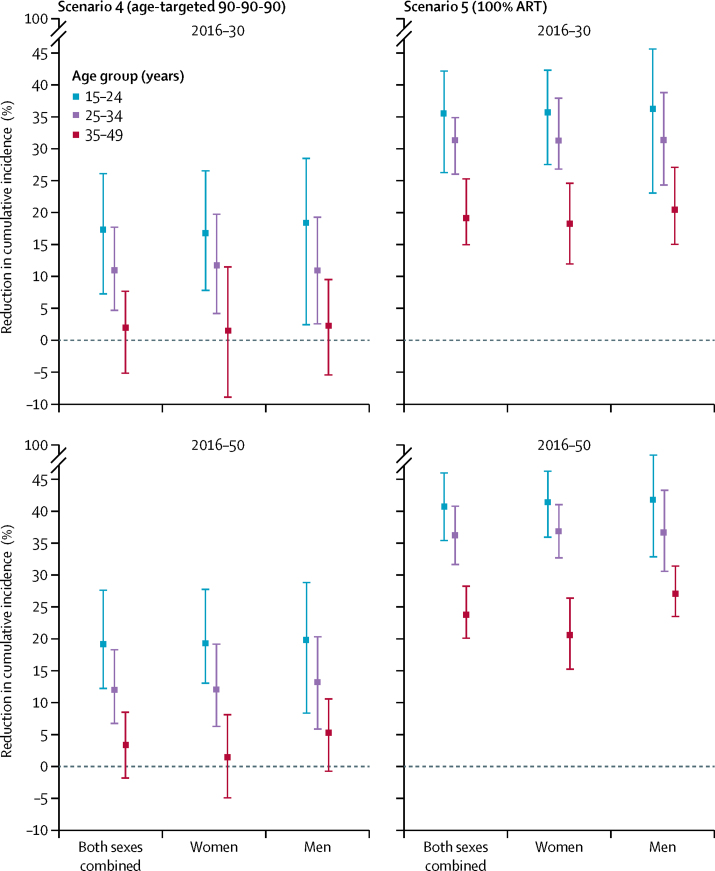
Findings: Between 2010 and 2016, status-quo ART scale-up among adults (aged 15-49 years) in eSwatini (from 34·0% in 2010 to 74·1% in 2016) reduced HIV incidence by 43·57% (95% credible interval 39·71 to 46·36) and HIV mortality by 56·17% (54·06 to 58·92) among individuals aged 15-49 years, with larger reductions in incidence among men and mortality among women. Holding 2016 ART coverage levels by age and sex into the future, by 2030 adult HIV incidence would fall to 1·09 (0·87 to 1·29) per 100 person-years, 1·42 (1·13 to 1·71) per 100 person-years among women and 0·79 (0·63 to 0·94) per 100 person-years among men. Achieving the 90-90-90 targets evenly by age and sex would further reduce incidence beyond status-quo ART, primarily among individuals aged 15-24 years (an additional 17·37% [7·33 to 26·12] reduction between 2016 and 2030), with only modest additional incidence reductions in adults aged 35-49 years (1·99% [-5·09 to 7·74]). Achieving 100% ART initiation among all people living with HIV within an average of 6 months from infection-an upper bound of plausible treatment effect-would reduce adult HIV incidence to 0·73 infections (0·55 to 0·92) per 100 person-years by 2030 and 0·46 (0·33 to 0·59) per 100 person-years by 2050.
Interpretation: Scale-up of ART over the last decade has already contributed to substantial reductions in HIV-1 incidence and mortality in eSwatini. Focused ART targeting would further reduce incidence, especially in younger individuals, but even the most aggressive treatment campaigns would be insufficient to end the epidemic in high-burden settings without a renewed focus on expanding preventive measures.
Funding: Global Good Fund and the Bill & Melinda Gates Foundation.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
How universal does universal test and treat have to be?Lancet HIV. 2020 May;7(5):e306-e308. doi: 10.1016/S2352-3018(20)30031-X. Epub 2020 Feb 13. Lancet HIV. 2020. PMID: 32061316 No abstract available.
Similar articles
-
Voluntary Medical Male Circumcision for HIV Prevention in Swaziland: Modeling the Impact of Age Targeting.PLoS One. 2016 Jul 13;11(7):e0156776. doi: 10.1371/journal.pone.0156776. eCollection 2016. PLoS One. 2016. PMID: 27410687 Free PMC article.
-
HIV incidence in western Kenya during scale-up of antiretroviral therapy and voluntary medical male circumcision: a population-based cohort analysis.Lancet HIV. 2018 May;5(5):e241-e249. doi: 10.1016/S2352-3018(18)30025-0. Epub 2018 Apr 9. Lancet HIV. 2018. PMID: 29650451
-
Impact and Cost of Scaling Up Voluntary Medical Male Circumcision for HIV Prevention in the Context of the New 90-90-90 HIV Treatment Targets.PLoS One. 2016 Oct 26;11(10):e0155734. doi: 10.1371/journal.pone.0155734. eCollection 2016. PLoS One. 2016. PMID: 27783681 Free PMC article.
-
Tuberculosis.In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. PMID: 30212088 Free Books & Documents. Review.
-
Getting to 90-90-90: Experiences from the MaxART Early Access to ART for All (EAAA) Trial in Eswatini.Curr HIV/AIDS Rep. 2020 Aug;17(4):324-332. doi: 10.1007/s11904-020-00501-6. Curr HIV/AIDS Rep. 2020. PMID: 32474844 Review.
Cited by
-
HIV Positive Pregnant Mothers' Perceptions and Experiences Regarding the Prevention of Mother-to-Child Transmission, Option B+ Program.J Patient Exp. 2021 Dec 6;8:23743735211065272. doi: 10.1177/23743735211065272. eCollection 2021. J Patient Exp. 2021. PMID: 34901413 Free PMC article.
-
The Impacts of Isolation Measures Against SARS-CoV-2 Infection on Sexual Health.AIDS Behav. 2020 Aug;24(8):2258-2259. doi: 10.1007/s10461-020-02853-x. AIDS Behav. 2020. PMID: 32246356 Free PMC article. No abstract available.
-
The impact of prevention-effective PrEP use on HIV incidence: a mathematical modelling study.J Int AIDS Soc. 2022 Nov;25(11):e26034. doi: 10.1002/jia2.26034. J Int AIDS Soc. 2022. PMID: 36385504 Free PMC article.
-
Future HIV epidemic trajectories in South Africa and projected long-term consequences of reductions in general population HIV testing: a mathematical modelling study.Lancet Public Health. 2024 Apr;9(4):e218-e230. doi: 10.1016/S2468-2667(24)00020-3. Lancet Public Health. 2024. PMID: 38553141 Free PMC article.
-
Viral suppression among pregnant adolescents and women living with HIV in rural KwaZulu-Natal, South Africa: a cross sectional study to assess progress towards UNAIDS indicators and Implications for HIV Epidemic Control.Reprod Health. 2022 May 12;19(1):116. doi: 10.1186/s12978-022-01419-5. Reprod Health. 2022. PMID: 35550580 Free PMC article.
References
-
- UNAIDS 90-90-90. An ambitious treatment target to help end the AIDS epidemic. 2014. https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
-
- Galvani AP, Pandey A, Fitzpatrick MC, Medlock J, Gray GE. Defining control of HIV epidemics. Lancet HIV. 2018;5:e667–e670. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
