

Inhaled corticosteroid withdrawal may improve outcomes in elderly patients with COPD exacerbation: a nationwide database study
- PMID: 32039260
- PMCID: PMC6995839
- DOI: 10.1183/23120541.00246-2019
Inhaled corticosteroid withdrawal may improve outcomes in elderly patients with COPD exacerbation: a nationwide database study
Abstract
Background: Inhaled corticosteroids (ICSs) are used for advanced-stage chronic obstructive pulmonary disease (COPD). The application and safety of ICS withdrawal remain controversial.This study aimed to evaluate the association between ICS withdrawal and outcomes in elderly patients with COPD with or without comorbid bronchial asthma, who were hospitalised for exacerbation.
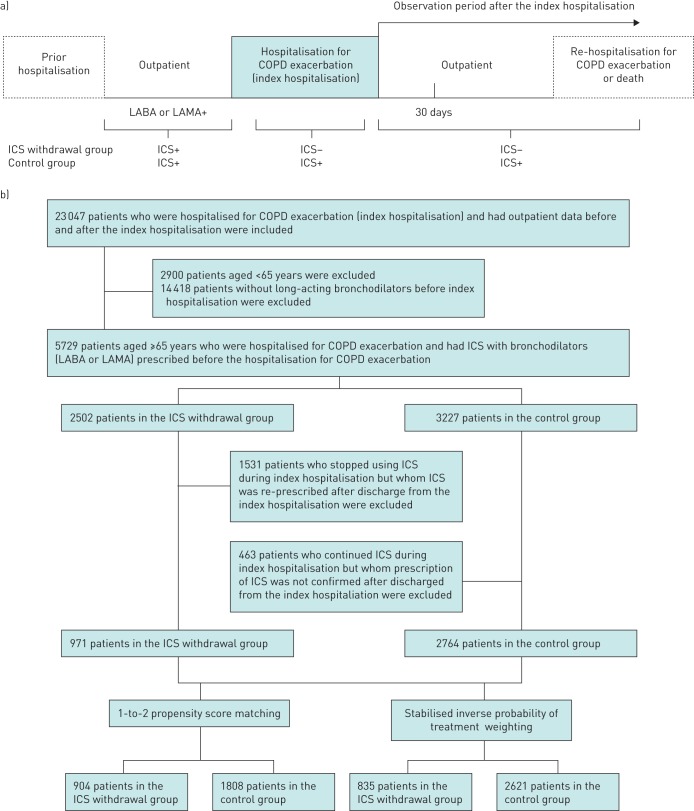
Patients and methods: We conducted a retrospective cohort study using the Japanese Diagnosis Procedure Combination database from July 2010 to March 2016. We identified patients aged ≥65 years who were hospitalised for COPD exacerbation. Re-hospitalisation for COPD exacerbation or death, frequency of antimicrobial medicine prescriptions and frequency of oral corticosteroid prescriptions after discharge were compared between patients with withdrawal and continuation of ICSs using propensity score analyses, namely 1-2 propensity score matching and stabilised inverse probability of treatment weighting.
Results: Among 3735 eligible patients, 971 and 2764 patients had ICS withdrawal and continuation, respectively. The hazard ratios (95% confidence intervals) of re-hospitalisation for COPD exacerbation or death for ICS withdrawal compared to continuation were 0.65 (0.52-0.80) in the propensity score matching and 0.71 (0.56-0.90) in the inverse probability of treatment weighting. The frequency of antimicrobial prescriptions but not corticosteroid prescriptions within 1 year was significantly less in the ICS withdrawal group. Among patients with comorbid bronchial asthma, ICS withdrawal was significantly associated with reduced re-hospitalisation for COPD exacerbation or death only in the propensity score matching analysis.
Conclusion: ICS withdrawal after COPD exacerbation was significantly associated with reduced incidences of re-hospitalisation or death among elderly patients, including those with comorbid bronchial asthma.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: T. Jo has nothing to disclose. Conflict of interest: H. Yasunaga reports grants from Ministry of Health, Labour, and Welfare, Japan, during the conduct of the study. Conflict of interest: Y. Yamauchi has nothing to disclose. Conflict of interest: A. Mitani has nothing to disclose. Conflict of interest: Y. Hiraishi has nothing to disclose. Conflict of interest: W. Hasegawa has nothing to disclose. Conflict of interest: Y. Sakamoto has nothing to disclose. Conflict of interest: H. Matsui has nothing to disclose. Conflict of interest: K. Fushimi has nothing to disclose. Conflict of interest: T. Nagase has nothing to disclose.
Figures

Similar articles
-
Comparative Effectiveness and Safety of Different Types of Inhaled Long-Acting β2-Agonist Plus Inhaled Long-Acting Muscarinic Antagonist vs Inhaled Long-Acting β2-Agonist Plus Inhaled Corticosteroid Fixed-Dose Combinations in COPD A Propensity Score-Inverse Probability of Treatment Weighting Cohort Study.Chest. 2021 Oct;160(4):1255-1270. doi: 10.1016/j.chest.2021.05.025. Epub 2021 May 21. Chest. 2021. PMID: 34023320
-
The Clinical Course of Asthma After Withdrawal of Inhaled Corticosteroids.J Allergy Clin Immunol Pract. 2021 Mar;9(3):1295-1303.e3. doi: 10.1016/j.jaip.2020.09.056. Epub 2020 Oct 10. J Allergy Clin Immunol Pract. 2021. PMID: 33049393
-
Economic assessment of early initiation of inhaled corticosteroids in chronic obstructive pulmonary disease using propensity score matching.Clin Ther. 2008;30 Spec No:1003-16. doi: 10.1016/j.clinthera.2008.05.020. Clin Ther. 2008. PMID: 18640475
-
Systematic review of inhaled corticosteroid withdrawal effects in chronic obstructive pulmonary disease, and comparison with two "real-life" studies.J Thorac Dis. 2018 Jul;10(7):4565-4573. doi: 10.21037/jtd.2018.06.151. J Thorac Dis. 2018. PMID: 30174909 Free PMC article. Review.
-
Effects of inhaled corticosteroids on mortality and hospitalisation in elderly asthma and chronic obstructive pulmonary disease patients: appraising the evidence.Drugs Aging. 2005;22(9):717-29. doi: 10.2165/00002512-200522090-00001. Drugs Aging. 2005. PMID: 16156676 Review.
Cited by
-
Corticosteroid use with extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest: A nationwide observational study.Resusc Plus. 2022 Sep 24;12:100308. doi: 10.1016/j.resplu.2022.100308. eCollection 2022 Dec. Resusc Plus. 2022. PMID: 36187432 Free PMC article.
-
Current developments and future directions in COPD.Eur Respir Rev. 2020 Dec 2;29(158):200289. doi: 10.1183/16000617.0289-2020. Print 2020 Dec 31. Eur Respir Rev. 2020. PMID: 33268439 Free PMC article.
-
Withdrawal of inhaled corticosteroids versus continuation of triple therapy in patients with COPD in real life: observational comparative effectiveness study.Respir Res. 2021 Jan 21;22(1):25. doi: 10.1186/s12931-021-01615-0. Respir Res. 2021. PMID: 33478491 Free PMC article.
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2019 Report. https://goldcopd.org/ Date last accessed: August 2, 2019 Date last updated: 2019.
-
- A joint project of GINA and GOLD: asthma, COPD, and asthma-COPD overlap syndrome (ACOS) https://goldcopd.org/asthma-copd-asthma-copd-overlap-syndrome/ Date last accessed: August 2, 2019. Date last updated: 2015.
LinkOut - more resources
Full Text Sources