

Case reports of a c.475G>T, p.E159* lamin A/C mutation with a family history of conduction disorder, dilated cardiomyopathy and sudden cardiac death
- PMID: 31847799
- PMCID: PMC6918565
- DOI: 10.1186/s12872-019-01282-6
Case reports of a c.475G>T, p.E159* lamin A/C mutation with a family history of conduction disorder, dilated cardiomyopathy and sudden cardiac death
Abstract
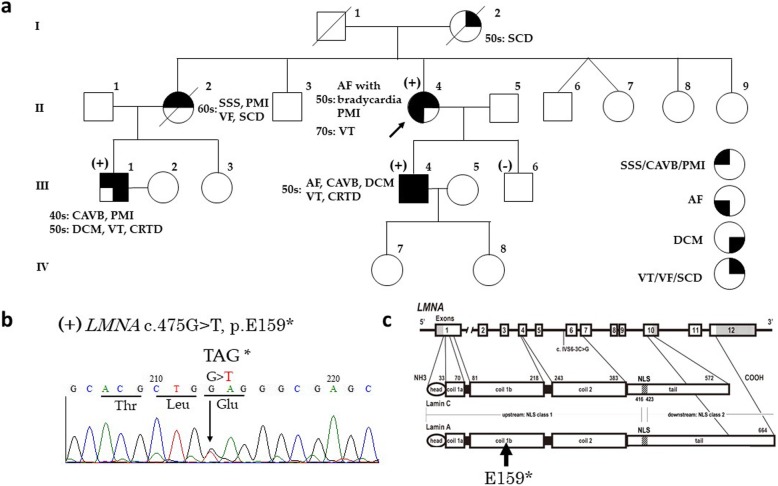
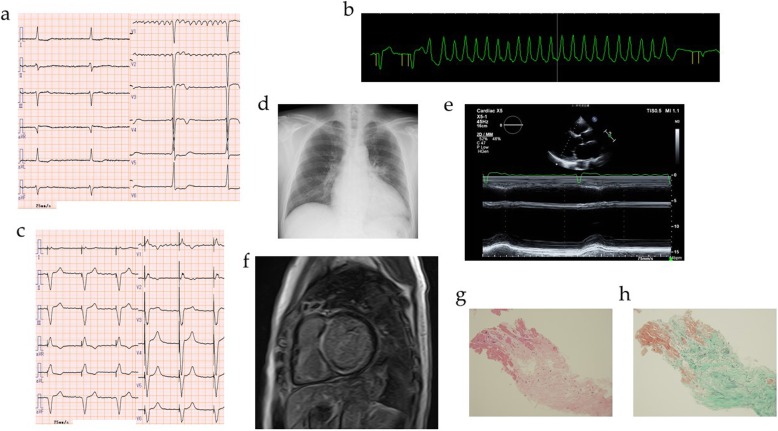
Background: Patients with some mutations in the lamin A/C (LMNA) gene are characterized by the presence of dilated cardiomyopathy (DCM), conduction abnormalities, ventricular tachyarrhythmias (VT), and sudden cardiac death (SCD). Various clinical features have been observed among patients who have the same LMNA mutation. Here, we show a family with cardiac laminopathy with a c.475G > T, p.E159* LMNA mutation, and a family history of conduction disorder, DCM, VT, and SCD.
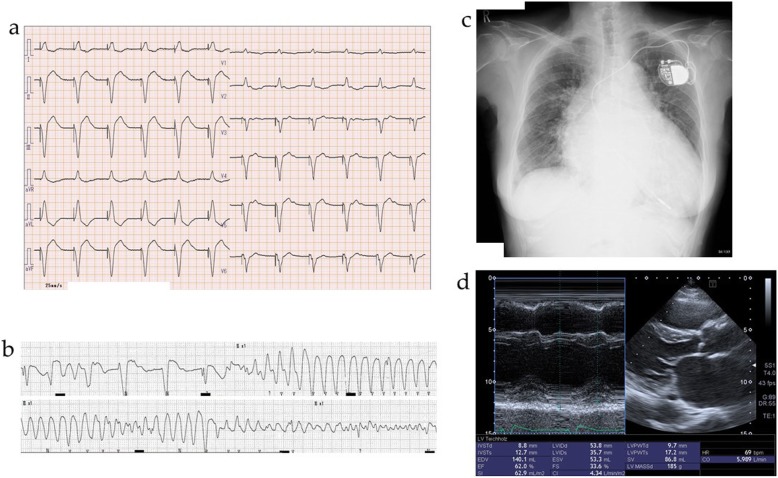
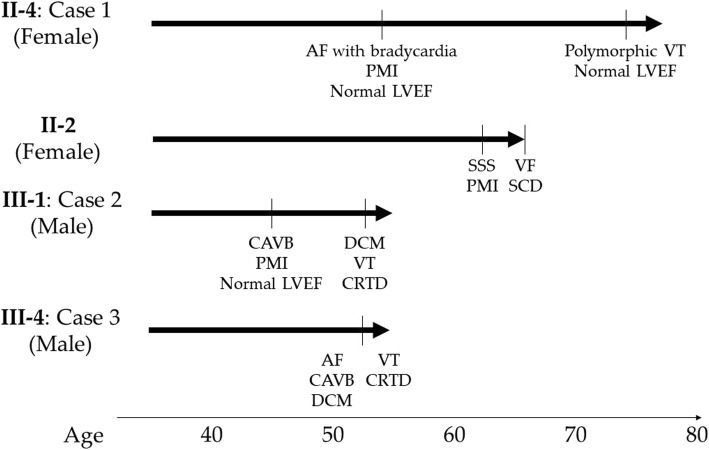
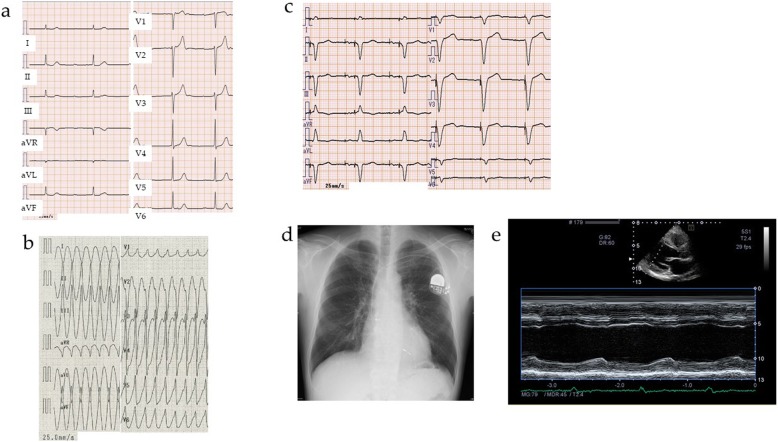
Case presentation: A proband (female) with atrial fibrillation and bradycardia was implanted with a pacemaker in her fifties. Twenty years later, she experienced a loss of consciousness due to polymorphic VT. She had a serious family history; her mother and elder sister died suddenly in their fifties and sixties, respectively, and her nephew and son were diagnosed as having DCM. Genetic screening of the proband, her son, and nephew identified a nonsense mutation (c.475G > T, p.E159*) in the LMNA gene. Although the proband's left ventricular ejection fraction remained relatively preserved, her son and nephew's left ventricular ejection fraction were reduced, resulting in cardiac resynchronization therapy by implantation of a defibrillator.
Conclusions: In this family with cardiac laminopathy with a c.475G > T, p.E159* LMNA mutation, DCM, SCD, and malignant VT occurred. Clinical manifestation of various atrial and ventricular arrhythmias and heart failure with reduced ejection fraction occurred in an age-dependent manner in all family members who had the nonsense mutation. It appears highly likely that the E159* LMNA mutation is related to various cardiac problems in the family of the current report.
Keywords: Case report; Dilated cardiomyopathy; Lamin A/C; Sudden cardiac death; c.475G > T; p.E159*.
Conflict of interest statement
Tetsuro Yokokawa belongs to a department supported by Actelion Pharmaceuticals Japan. Takashi Kaneshiro belongs to a department supported by Biotronic Japan and Abbot Japan. Akiomi Yoshihisa belongs to a department supported by Fukuda Denshi Co. Ltd. These companies were not associated with the contents of this study.
Figures
Similar articles
-
A novel LMNA nonsense mutation causes two distinct phenotypes of cardiomyopathy with high risk of sudden cardiac death in a large five-generation family.Europace. 2018 Dec 1;20(12):2003-2013. doi: 10.1093/europace/euy127. Europace. 2018. PMID: 29947763
-
Implantable cardioverter-defibrillators in lamin A/C mutation carriers with cardiac conduction disorders.Heart Rhythm. 2013 Oct;10(10):1492-8. doi: 10.1016/j.hrthm.2013.06.020. Epub 2013 Jun 26. Heart Rhythm. 2013. PMID: 23811080
-
Clinical and functional characterization of a novel mutation in lamin a/c gene in a multigenerational family with arrhythmogenic cardiac laminopathy.PLoS One. 2015 Apr 2;10(4):e0121723. doi: 10.1371/journal.pone.0121723. eCollection 2015. PLoS One. 2015. PMID: 25837155 Free PMC article.
-
Laminopathies: a Pandora's box of heart failure, bradyarrhythmias and sudden death.Rev Port Cardiol. 2015 Feb;34(2):139.e1-5. doi: 10.1016/j.repc.2014.08.007. Epub 2015 Feb 3. Rev Port Cardiol. 2015. PMID: 25656816 Review. English, Portuguese.
-
Lamin A/C mutations in dilated cardiomyopathy.Cardiol J. 2014;21(4):331-42. doi: 10.5603/CJ.a2014.0037. Epub 2014 May 20. Cardiol J. 2014. PMID: 24846508 Review.
Cited by
-
Atrial fibrillation.Nat Rev Dis Primers. 2016 Mar 31;2:16017. doi: 10.1038/nrdp.2016.17. Nat Rev Dis Primers. 2016. PMID: 27227428 Free PMC article.
-
Inherited and Acquired Rhythm Disturbances in Sick Sinus Syndrome, Brugada Syndrome, and Atrial Fibrillation: Lessons from Preclinical Modeling.Cells. 2021 Nov 15;10(11):3175. doi: 10.3390/cells10113175. Cells. 2021. PMID: 34831398 Free PMC article. Review.
-
Novel pathogenic variant in LMNA gene identified in a six-generation family causing atrial cardiomyopathy and associated right atrial conduction arrhythmias.Front Cardiovasc Med. 2023 Jul 3;10:1109008. doi: 10.3389/fcvm.2023.1109008. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37465451 Free PMC article.
-
Cardiac conduction diseases: understanding the molecular mechanisms to uncover targets for future treatments.Expert Opin Ther Targets. 2024 May;28(5):385-400. doi: 10.1080/14728222.2024.2351501. Epub 2024 May 13. Expert Opin Ther Targets. 2024. PMID: 38700451 Review.
-
Cytoskeletal Protein Variants Driving Atrial Fibrillation: Potential Mechanisms of Action.Cells. 2022 Jan 25;11(3):416. doi: 10.3390/cells11030416. Cells. 2022. PMID: 35159226 Free PMC article. Review.
References
-
- Arbustini E, Pilotto A, Repetto A, Grasso M, Negri A, Diegoli M, Campana C, Scelsi L, Baldini E, Gavazzi A, Tavazzi L. Autosomal dominant dilated cardiomyopathy with atrioventricular block: a Lamin a/C defect-related disease. J Am Coll Cardiol. 2002;39:981–990. doi: 10.1016/S0735-1097(02)01724-2. - DOI - PubMed
-
- Taylor MR, Fain PR, Sinagra G, Robinson ML, Robertson AD, Carniel E, Di Lenarda A, Bohlmeyer TJ, Ferguson DA, Brodsky GL, Boucek MM, Lascor J, Moss AC, Li WL, Stetler GL, et al. Natural history of dilated cardiomyopathy due to Lamin A/C gene mutations. J Am Coll Cardiol. 2003;41:771–780. doi: 10.1016/S0735-1097(02)02954-6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
