

Treg cell-based therapies: challenges and perspectives
- PMID: 31811270
- PMCID: PMC7814338
- DOI: 10.1038/s41577-019-0232-6
Treg cell-based therapies: challenges and perspectives
Abstract
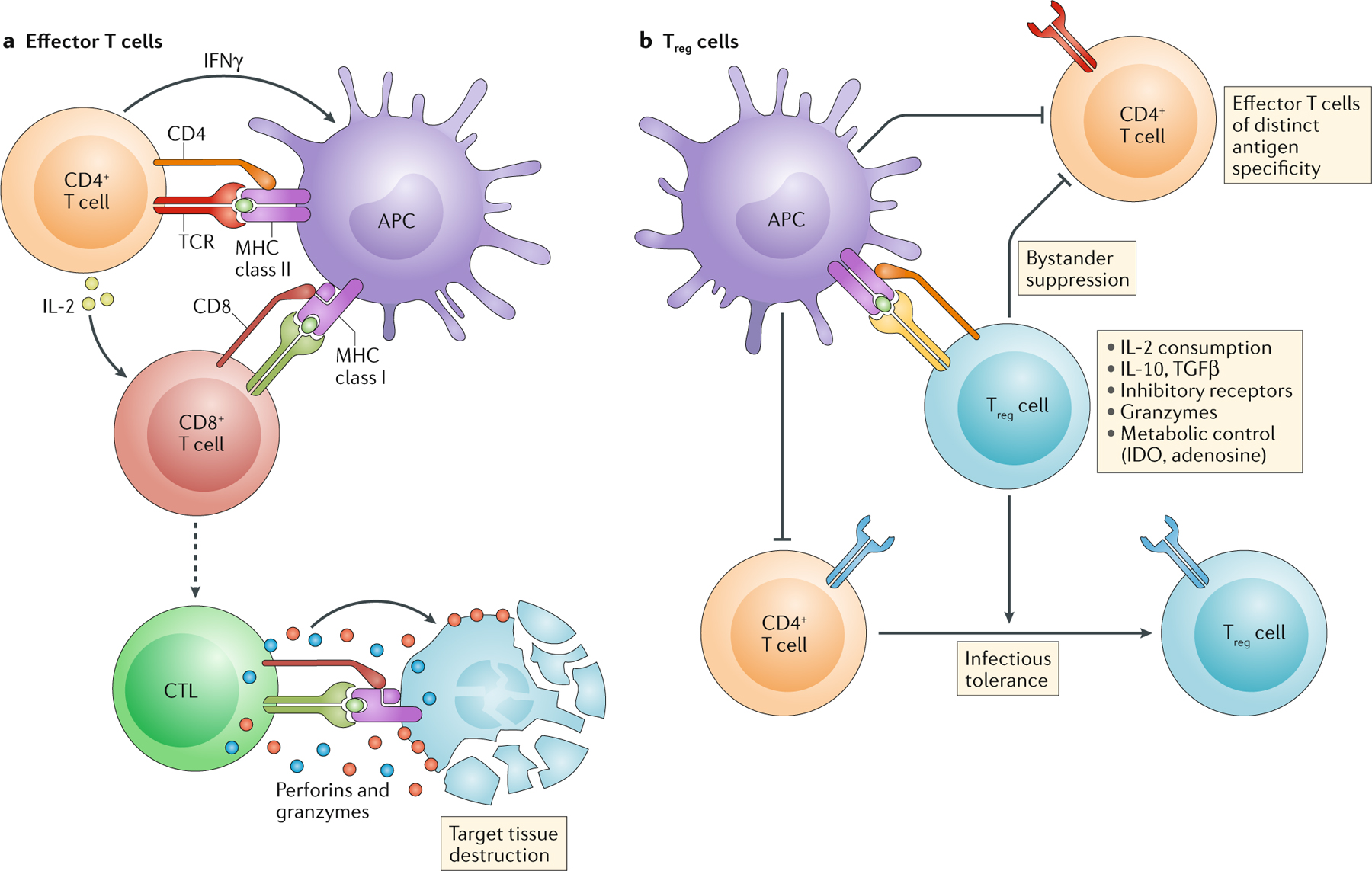
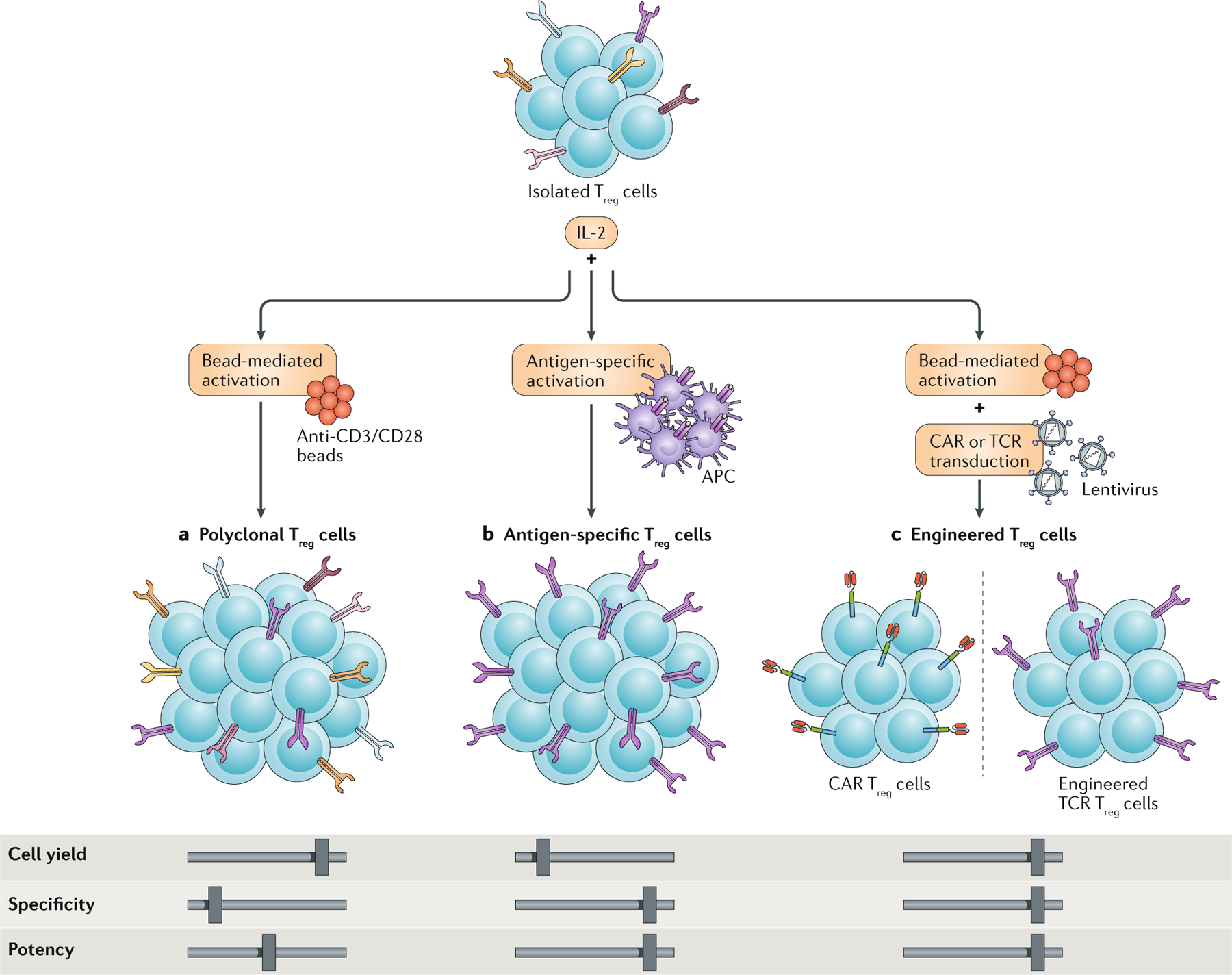
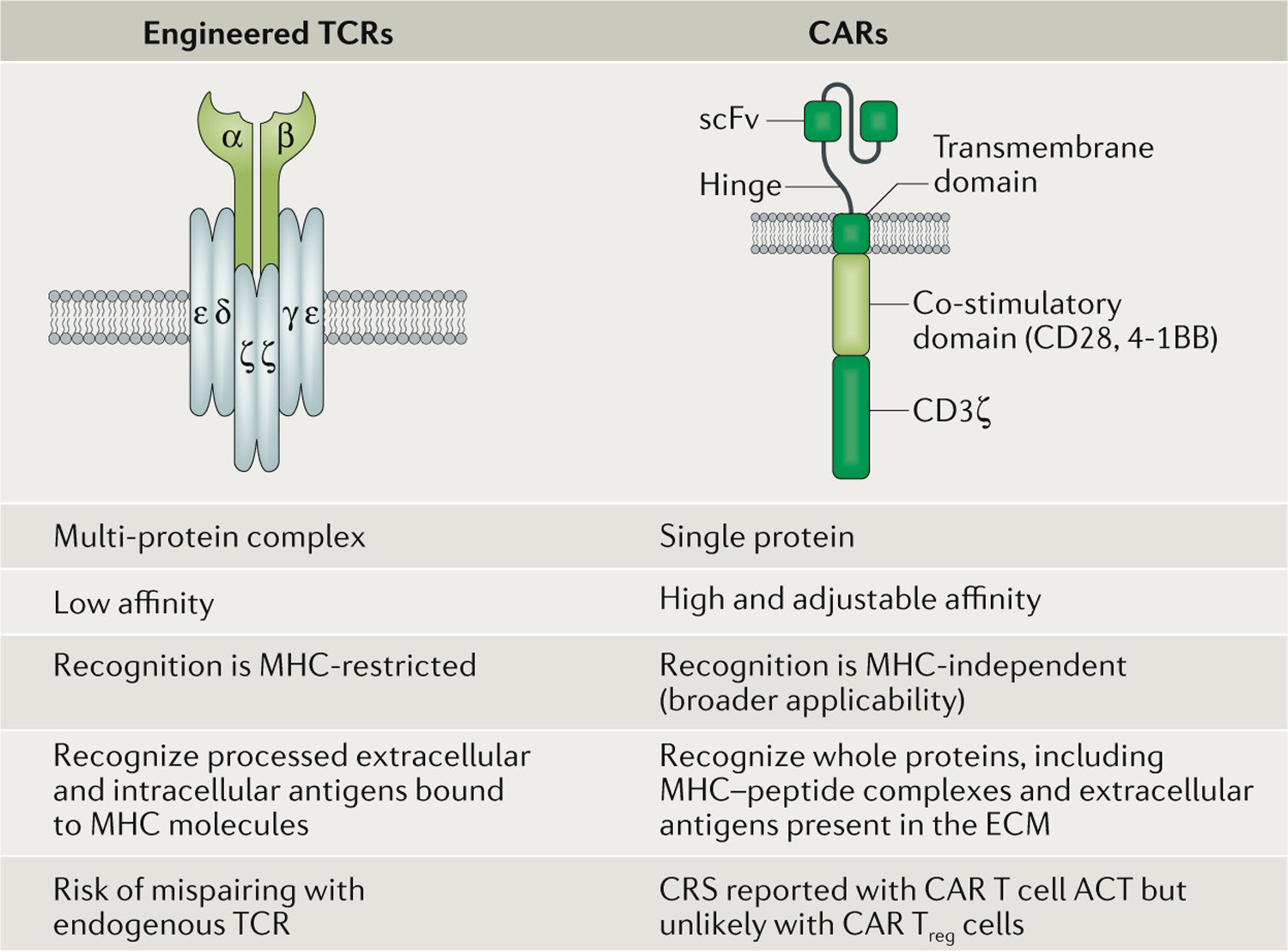
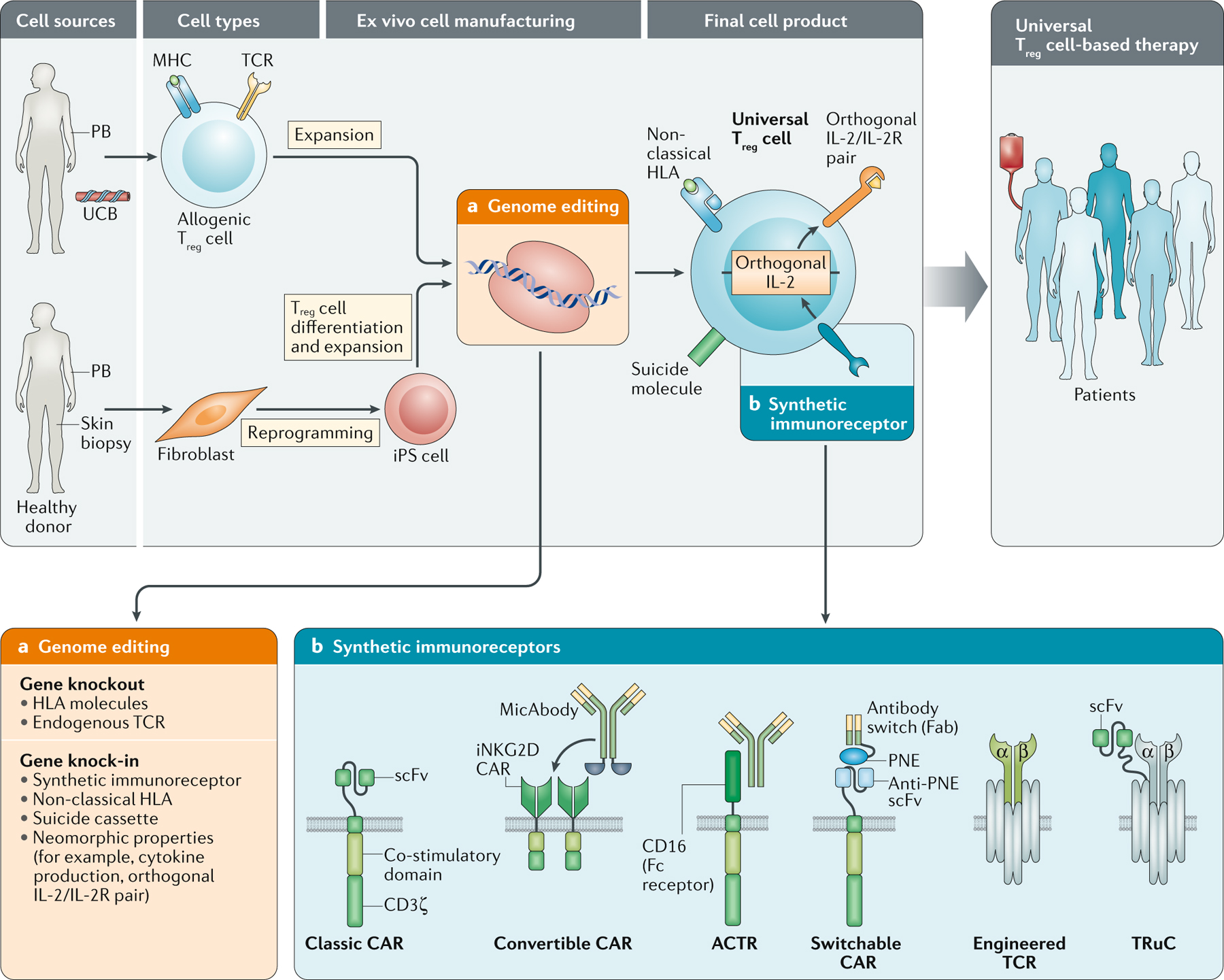
Cellular therapies using regulatory T (Treg) cells are currently undergoing clinical trials for the treatment of autoimmune diseases, transplant rejection and graft-versus-host disease. In this Review, we discuss the biology of Treg cells and describe new efforts in Treg cell engineering to enhance specificity, stability, functional activity and delivery. Finally, we envision that the success of Treg cell therapy in autoimmunity and transplantation will encourage the clinical use of adoptive Treg cell therapy for non-immune diseases, such as neurological disorders and tissue repair.
Conflict of interest statement
Competing interests
J.A.B. is a stock holder and member of the Board of Directors on Rheos Medicines; a stock holder and member of the Board of Directors for Provention Bio; and a stock holder and member of the Scientific Advisory Boards of Vir Therapeutics, Arcus Biotherapeutics, Quentis Therapeutics, Solid Biosciences and Celsius Therapeutics (Founder). J.A.B. owns stock in MacroGenics Inc., Vir Therapeutics, Arcus Biotherapeutics, Quentis Therapeutics, Solid Biosciences and Celsius Therapeutics. C.R. and L.T.V. declare no competing interests. J.A.B is the President and CEO of a newly formed biotech company targeting Treg therapy for the treatment of autoimmune and other immune disorders.
Figures
Similar articles
-
Antigen-Specific Regulatory T Cell Therapy in Autoimmune Diseases and Transplantation.Front Immunol. 2021 May 14;12:661875. doi: 10.3389/fimmu.2021.661875. eCollection 2021. Front Immunol. 2021. PMID: 34054826 Free PMC article. Review.
-
Next-generation regulatory T cell therapy.Nat Rev Drug Discov. 2019 Oct;18(10):749-769. doi: 10.1038/s41573-019-0041-4. Epub 2019 Sep 20. Nat Rev Drug Discov. 2019. PMID: 31541224 Free PMC article. Review.
-
The Next Frontier of Regulatory T Cells: Promising Immunotherapy for Autoimmune Diseases and Organ Transplantations.Front Immunol. 2020 Sep 23;11:565518. doi: 10.3389/fimmu.2020.565518. eCollection 2020. Front Immunol. 2020. PMID: 33072105 Free PMC article. Review.
-
Separating the wheat from the chaff: Making sense of Treg heterogeneity for better adoptive cellular therapy.Immunol Lett. 2021 Nov;239:96-112. doi: 10.1016/j.imlet.2021.03.002. Epub 2021 Mar 4. Immunol Lett. 2021. PMID: 33676975 Review.
-
Engineered Treg cells: The heir to the throne of immunotherapy.J Autoimmun. 2024 Apr;144:102986. doi: 10.1016/j.jaut.2022.102986. Epub 2023 Jan 11. J Autoimmun. 2024. PMID: 36639301 Review.
Cited by
-
Human regulatory T cells locally differentiate and are functionally heterogeneous within the inflamed arthritic joint.Clin Transl Immunology. 2022 Sep 30;11(10):e1420. doi: 10.1002/cti2.1420. eCollection 2022. Clin Transl Immunology. 2022. PMID: 36204213 Free PMC article.
-
A split, conditionally active mimetic of IL-2 reduces the toxicity of systemic cytokine therapy.Nat Biotechnol. 2023 Apr;41(4):532-540. doi: 10.1038/s41587-022-01510-z. Epub 2022 Oct 31. Nat Biotechnol. 2023. PMID: 36316485 Free PMC article.
-
Mechanisms of exTreg induction.Eur J Immunol. 2021 Aug;51(8):1956-1967. doi: 10.1002/eji.202049123. Epub 2021 May 27. Eur J Immunol. 2021. PMID: 33975379 Free PMC article. Review.
-
Augmenting regulatory T cells: new therapeutic strategy for rheumatoid arthritis.Front Immunol. 2024 Jan 23;15:1312919. doi: 10.3389/fimmu.2024.1312919. eCollection 2024. Front Immunol. 2024. PMID: 38322264 Free PMC article. Review.
-
[Genetically modified regulatory T cells: therapeutic concepts and regulatory aspects].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2020 Nov;63(11):1403-1411. doi: 10.1007/s00103-020-03230-8. Epub 2020 Oct 16. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2020. PMID: 33067665 Free PMC article. Review. German.
References
-
- Edinger M et al. CD4+CD25+ regulatory T cells preserve graft-versus-tumor activity while inhibiting graft-versus-host disease after bone marrow transplantation. Nat. Med 9, 1144–1150 (2003). - PubMed
-
- Taylor PA, Lees CJ & Blazar BR The infusion of ex vivo activated and expanded CD4+CD25+ immune regulatory cells inhibits graft-versus-host disease lethality. Blood 99, 3493–3499 (2002). - PubMed
-
- Xia G, He J & Leventhal JR Ex vivo-expanded natural CD4+CD25+ regulatory T cells synergize with host T-cell depletion to promote long-term survival of allografts. Am. J. Transpl 8, 298–306 (2008). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
