

Predominantly Antibody-Deficient Patients With Non-infectious Complications Have Reduced Naive B, Treg, Th17, and Tfh17 Cells
- PMID: 31803177
- PMCID: PMC6873234
- DOI: 10.3389/fimmu.2019.02593
Predominantly Antibody-Deficient Patients With Non-infectious Complications Have Reduced Naive B, Treg, Th17, and Tfh17 Cells
Abstract
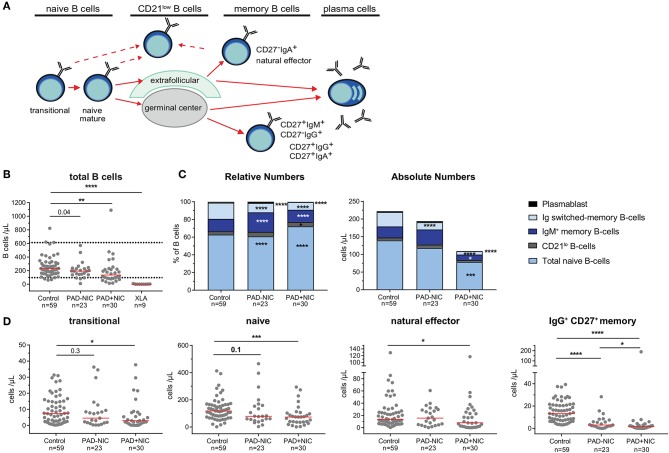
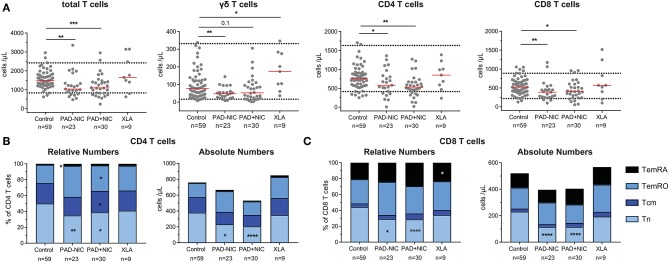
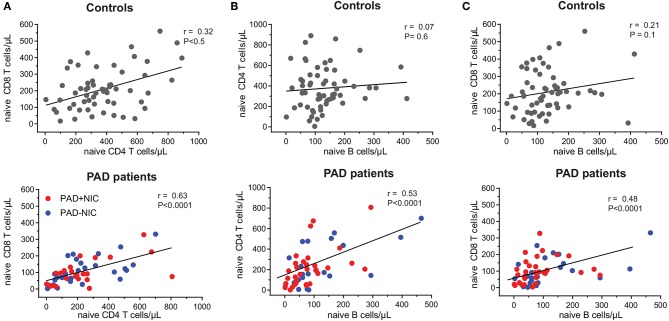
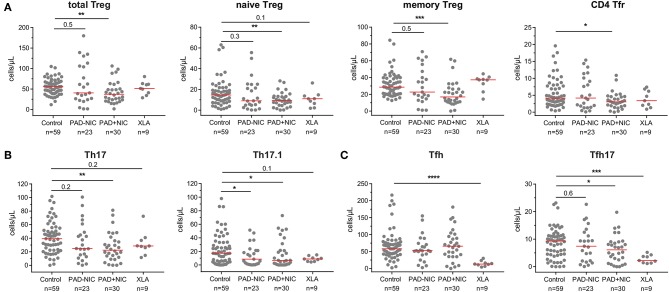
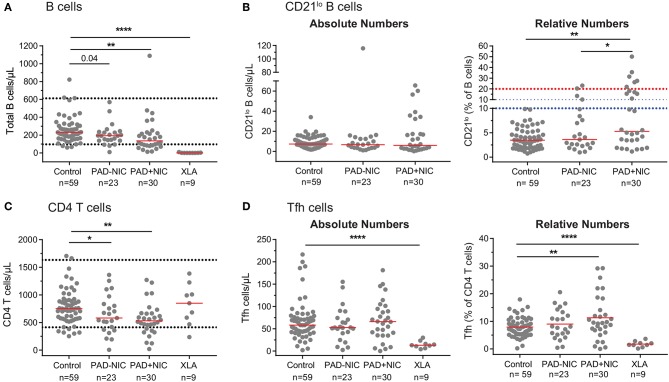
Background: Patients with predominantly antibody deficiency (PAD) suffer from severe and recurrent infections that require lifelong immunoglobulin replacement and prophylactic antibiotic treatment. Disease incidence is estimated to be 1:25,000 worldwide, and up to 68% of patients develop non-infectious complications (NIC) including autoimmunity, which are difficult to treat, causing high morbidity, and early mortality. Currently, the etiology of NIC is unknown, and there are no diagnostic and prognostic markers to identify patients at risk. Objectives: To identify immune cell markers that associate with NIC in PAD patients. Methods: We developed a standardized 11-color flow cytometry panel that was utilized for in-depth analysis of B and T cells in 62 adult PAD patients and 59 age-matched controls. Results: Nine males had mutations in Bruton's tyrosine kinase (BTK) and were defined as having X-linked agammaglobulinemia. The remaining 53 patients were not genetically defined and were clinically diagnosed with agammaglobulinemia (n = 1), common variable immunodeficiency (CVID) (n = 32), hypogammaglobulinemia (n = 13), IgG subclass deficiency (n = 1), and specific polysaccharide antibody deficiency (n = 6). Of the 53, 30 (57%) had one or more NICs, 24 patients had reduced B-cell numbers, and 17 had reduced T-cell numbers. Both PAD-NIC and PAD+NIC groups had significantly reduced Ig class-switched memory B cells and naive CD4 and CD8 T-cell numbers. Naive and IgM memory B cells, Treg, Th17, and Tfh17 cells were specifically reduced in the PAD+NIC group. CD21lo B cells and Tfh cells were increased in frequencies, but not in absolute numbers in PAD+NIC. Conclusion: The previously reported increased frequencies of CD21lo B cells and Tfh cells are the indirect result of reduced naive B-cell and T-cell numbers. Hence, correct interpretation of immunophenotyping of immunodeficiencies is critically dependent on absolute cell counts. Finally, the defects in naive B- and T-cell numbers suggest a mild combined immunodeficiency in PAD patients with NIC. Together with the reductions in Th17, Treg, and Tfh17 numbers, these key differences could be utilized as biomarkers to support definitive diagnosis and to predict for disease progression.
Keywords: CD21lo B cells; EuroFlow; X-linked agammaglobulinemia; autoimmunity; common variable immunodeficiency; follicular helper T cells; naive T cells; predominantly antibody deficiency.
Copyright © 2019 Edwards, Bosco, Aui, Stirling, Cameron, Chatelier, Hore-Lacy, O'Hehir and van Zelm.
Figures
Similar articles
-
The immunophenotypic fingerprint of patients with primary antibody deficiencies is partially present in their asymptomatic first-degree relatives.Haematologica. 2017 Jan;102(1):192-202. doi: 10.3324/haematol.2016.149112. Epub 2016 Sep 15. Haematologica. 2017. PMID: 27634199 Free PMC article.
-
Defects in memory B-cell and plasma cell subsets expressing different immunoglobulin-subclasses in patients with CVID and immunoglobulin subclass deficiencies.J Allergy Clin Immunol. 2019 Sep;144(3):809-824. doi: 10.1016/j.jaci.2019.02.017. Epub 2019 Feb 28. J Allergy Clin Immunol. 2019. PMID: 30826363
-
T cell phenotypes in patients with common variable immunodeficiency disorders: associations with clinical phenotypes in comparison with other groups with recurrent infections.Clin Exp Immunol. 2012 Nov;170(2):202-11. doi: 10.1111/j.1365-2249.2012.04643.x. Clin Exp Immunol. 2012. PMID: 23039891 Free PMC article.
-
Regulatory T cells and T helper 17 cells in viral infection.Scand J Immunol. 2020 May;91(5):e12873. doi: 10.1111/sji.12873. Epub 2020 Mar 10. Scand J Immunol. 2020. PMID: 32090360 Review.
-
The plasticity of human Treg and Th17 cells and its role in autoimmunity.Semin Immunol. 2013 Nov 15;25(4):305-12. doi: 10.1016/j.smim.2013.10.009. Epub 2013 Nov 5. Semin Immunol. 2013. PMID: 24211039 Free PMC article. Review.
Cited by
-
Long-Term Immunological Memory of SARS-CoV-2 Is Present in Patients with Primary Antibody Deficiencies for up to a Year after Vaccination.Vaccines (Basel). 2023 Feb 3;11(2):354. doi: 10.3390/vaccines11020354. Vaccines (Basel). 2023. PMID: 36851231 Free PMC article.
-
Wenyang Huazhuo Tuihuang Formula Inhibits the Th17/Treg Cell Imbalance and Protects against Acute-on-Chronic Liver Failure.Evid Based Complement Alternat Med. 2022 Mar 30;2022:5652172. doi: 10.1155/2022/5652172. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35399641 Free PMC article.
-
Patients with Common Variable Immunodeficiency Complicated by Autoimmune Phenomena Have Lymphopenia and Reduced Treg, Th17, and NK Cells.J Clin Med. 2021 Jul 29;10(15):3356. doi: 10.3390/jcm10153356. J Clin Med. 2021. PMID: 34362140 Free PMC article.
-
Increased Th22 cell numbers in a general pediatric population with filaggrin haploinsufficiency: The Generation R Study.Pediatr Allergy Immunol. 2021 Aug;32(6):1360-1368. doi: 10.1111/pai.13502. Epub 2021 Mar 29. Pediatr Allergy Immunol. 2021. PMID: 33715246 Free PMC article.
-
Influenza-specific IgG1+ memory B-cell numbers increase upon booster vaccination in healthy adults but not in patients with predominantly antibody deficiency.Clin Transl Immunology. 2020 Oct 16;9(10):e1199. doi: 10.1002/cti2.1199. eCollection 2020. Clin Transl Immunology. 2020. PMID: 33088507 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials