

Zika virus infection as a cause of congenital brain abnormalities and Guillain-Barré syndrome: A living systematic review
- PMID: 31754425
- PMCID: PMC6852328
- DOI: 10.12688/f1000research.19918.1
Zika virus infection as a cause of congenital brain abnormalities and Guillain-Barré syndrome: A living systematic review
Abstract
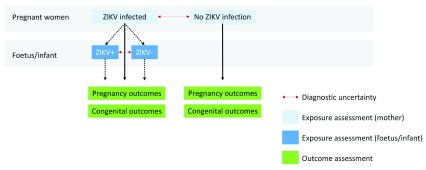
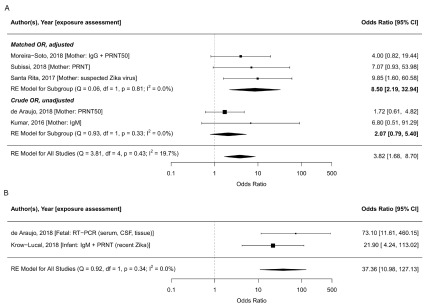
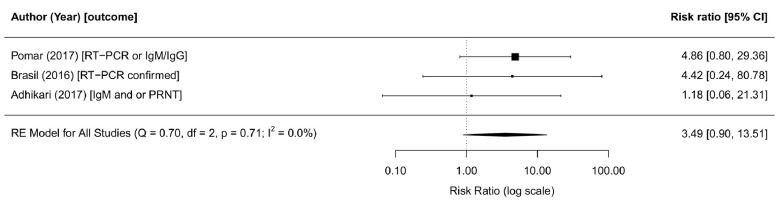
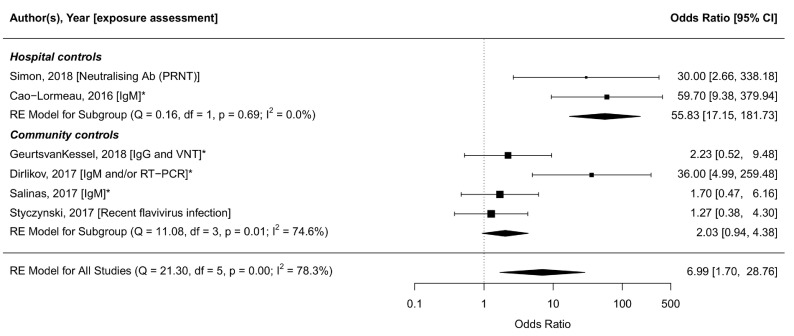
Background: The Zika virus (ZIKV) caused a large outbreak in the Americas leading to the declaration of a Public Health Emergency of International Concern in February 2016. A causal relation between infection and adverse congenital outcomes such as microcephaly was declared by the World Health Organization (WHO) informed by a systematic review structured according to a framework of ten dimensions of causality, based on the work of Bradford Hill. Subsequently, the evidence has continued to accumulate, which we incorporate in regular updates of the original work, rendering it a living systematic review. Methods: We present an update of our living systematic review on the causal relation between ZIKV infection and adverse congenital outcomes and between ZIKV and GBS for four dimensions of causality: strength of association, dose-response, specificity, and consistency. We assess the evidence published between January 18, 2017 and July 1, 2019. Results: We found that the strength of association between ZIKV infection and adverse outcomes from case-control studies differs according to whether exposure to ZIKV is assessed in the mother (OR 3.8, 95% CI: 1.7-8.7, I 2=19.8%) or the foetus/infant (OR 37.4, 95% CI: 11.0-127.1, I 2=0%). In cohort studies, the risk of congenital abnormalities was 3.5 times higher after ZIKV infection (95% CI: 0.9-13.5, I 2=0%). The strength of association between ZIKV infection and GBS was higher in studies that enrolled controls from hospital (OR: 55.8, 95% CI: 17.2-181.7, I 2=0%) than in studies that enrolled controls at random from the same community or household (OR: 2.0, 95% CI: 0.8-5.4, I 2=74.6%). In case-control studies, selection of controls from hospitals could have biased results. Conclusions: The conclusions that ZIKV infection causes adverse congenital outcomes and GBS are reinforced with the evidence published between January 18, 2017 and July 1, 2019.
Keywords: Disease outbreaks; Guillain-Barré syndrome; Zika; arboviruses; causality; congenital abnormalities.
Copyright: © 2019 Counotte MJ et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
Similar articles
-
Zika virus infection as a cause of congenital brain abnormalities and Guillain-Barré syndrome: From systematic review to living systematic review.F1000Res. 2018 Feb 15;7:196. doi: 10.12688/f1000research.13704.1. eCollection 2018. F1000Res. 2018. PMID: 30631437 Free PMC article.
-
Zika Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain-Barré Syndrome: Systematic Review.PLoS Med. 2017 Jan 3;14(1):e1002203. doi: 10.1371/journal.pmed.1002203. eCollection 2017 Jan. PLoS Med. 2017. PMID: 28045901 Free PMC article. Review.
-
Neurological complications of Zika virus infection.Expert Rev Anti Infect Ther. 2018 May;16(5):399-410. doi: 10.1080/14787210.2018.1466702. Epub 2018 Apr 26. Expert Rev Anti Infect Ther. 2018. PMID: 29668332 Review.
-
Zika virus infection: epidemiology, clinical manifestations and diagnosis.Curr Opin Infect Dis. 2016 Oct;29(5):459-66. doi: 10.1097/QCO.0000000000000301. Curr Opin Infect Dis. 2016. PMID: 27496713 Review.
-
Health outcomes associated with Zika virus infection in humans: a systematic review of systematic reviews.BMJ Open. 2019 Nov 3;9(11):e032275. doi: 10.1136/bmjopen-2019-032275. BMJ Open. 2019. PMID: 31685512 Free PMC article.
Cited by
-
Prevalence and Mortality of Pediatrics with Guillain-Barré Syndrome during the COVID-19 Pandemic and Pre-COVID-19 Periods.Iran J Child Neurol. 2024 Fall;18(4):71-79. doi: 10.22037/ijcn.v18i4.43818. Epub 2024 Sep 29. Iran J Child Neurol. 2024. PMID: 39478952 Free PMC article.
-
Zika virus-like particle vaccine fusion loop mutation increases production yield but fails to protect AG129 mice against Zika virus challenge.PLoS Negl Trop Dis. 2022 Jul 6;16(7):e0010588. doi: 10.1371/journal.pntd.0010588. eCollection 2022 Jul. PLoS Negl Trop Dis. 2022. PMID: 35793354 Free PMC article.
-
Memantine treatment reduces the incidence of flaccid paralysis in a zika virus mouse model of temporary paralysis with similarities to Guillain-Barré syndrome.Antivir Chem Chemother. 2020 Jan-Dec;28:2040206620950143. doi: 10.1177/2040206620950143. Antivir Chem Chemother. 2020. PMID: 34161179 Free PMC article.
-
Zika virus NS2A protein induces the degradation of KPNA2 (karyopherin subunit alpha 2) via chaperone-mediated autophagy.Autophagy. 2020 Dec;16(12):2238-2251. doi: 10.1080/15548627.2020.1823122. Epub 2020 Sep 28. Autophagy. 2020. PMID: 32924767 Free PMC article.
-
Zika virus-like particle vaccine protects AG129 mice and rhesus macaques against Zika virus.PLoS Negl Trop Dis. 2021 Mar 12;15(3):e0009195. doi: 10.1371/journal.pntd.0009195. eCollection 2021 Mar. PLoS Negl Trop Dis. 2021. PMID: 33711018 Free PMC article.