

Pacemaker Lead Endocarditis Investigated with Intracardiac Echocardiography: Factors Modulating the Size of Vegetations and Larger Vegetation Embolic Risk during Lead Extraction
- PMID: 31752363
- PMCID: PMC6963371
- DOI: 10.3390/antibiotics8040228
Pacemaker Lead Endocarditis Investigated with Intracardiac Echocardiography: Factors Modulating the Size of Vegetations and Larger Vegetation Embolic Risk during Lead Extraction
Abstract
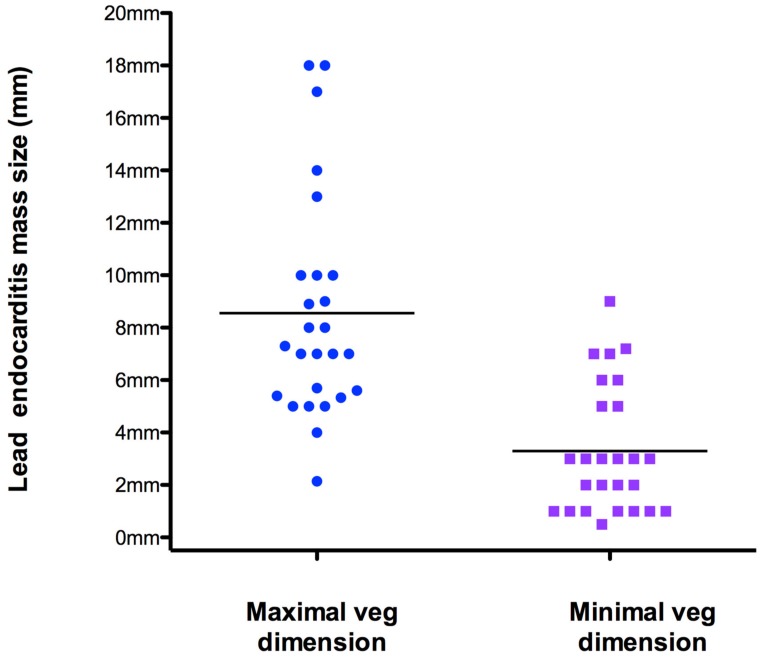
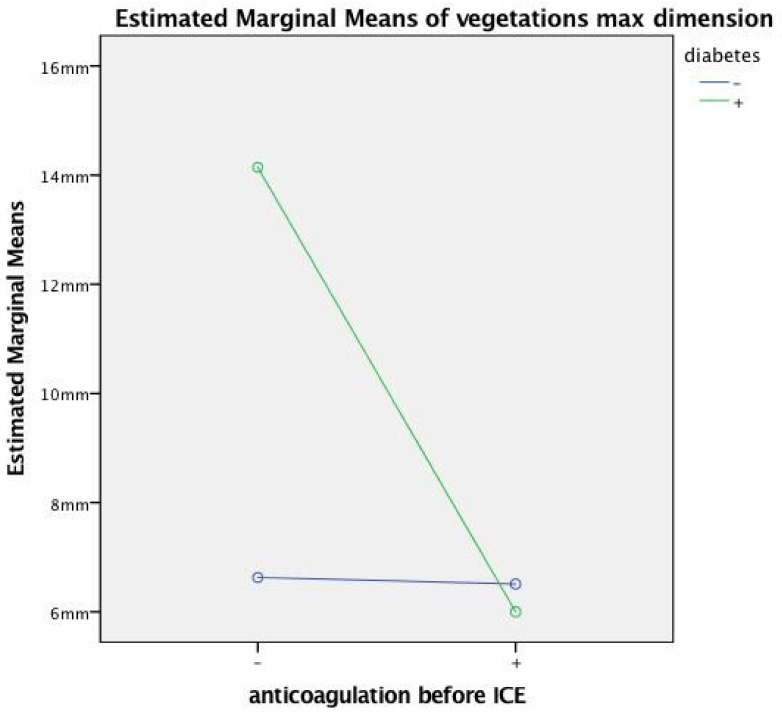
Lead pacemaker infection is a complication on the rise. An infected oscillating mass attached to the leads (ILV) is a common finding in this setting. Percutaneous extraction of the leads and of the device is the best curative option. However, extraction of leads with large masses can be complicated by pulmonary embolism. The aim of this study was to understand the factors associated with large ILV using a sophisticated ultrasound technique to visualize the masses, namely intracardiac echocardiography (ICE), and investigate whether larger masses induce more complications during and after extraction. Percutaneous lead extraction and peri-procedural ICE were done in 36 patients (pts) (75 ± 11 years old, 74% males). Vegetations (max dimension = 8.2 ± 4.1 mm) in the right cavity were found in 26 of them, mostly adhering to the leads. We subdivided the patients into 2 groups: with vegetation size < 1 cm (18 pts) and vegetation size ≥ 1 cm (8 pts). By univariate analysis, we found that patients in group 1 were more often taking anticoagulation therapy (p = 0.03, Phi (Phi coefficient) = -0.5, OR [odds ratio] 0.071) and had signs of local pocket infection (p = 0.02, Phi = -0.52, OR 0.059) while significantly more patients in group 2 had diabetes (p = 0.08, Phi = 0.566, OR 15); moreover the patients in group 2 showed a trend toward a more frequent positive blood culture (p = 0.08, Phi = 0.39, OR 5.8) and infection with coagulase negative staphylococci (p = 0.06, Phi = 0.46, OR 8.3). At multivariate analysis, only 3 factors (diabetes, younger age and anticoagulation therapy) were independently associated with ILV size: diabetes, associated with larger vegetations (group 2), showed the largest beta value (0.44, p = 0.008); age was inversely correlated with ILV size (beta value = -32, p = 0.038), and anticoagulation therapy (beta value = -029, p = 0.048) was more commonly associated with smaller vegetations (group 1). Larger ILV were not associated with more complications or death during or after the extraction. Conclusion: diabetes, anticoagulation therapy and age are independent predictors of lead vegetation size. The embolic potential of large ILV during extraction was modest, so ILVs >1cm are not a contraindication to percutaneous extraction of infected leads.
Keywords: embolism; infective endocarditis; intracardiac echocardiography; lead vegetations; pacemaker.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Lead-related infective endocarditis: factors influencing the formation of large vegetations.Europace. 2017 Jun 1;19(6):1022-1030. doi: 10.1093/europace/euw121. Europace. 2017. PMID: 27358071
-
Influence of vegetation shape on outcomes in transvenous lead extractions: Does shape matter?Heart Rhythm. 2020 Apr;17(4):646-653. doi: 10.1016/j.hrthm.2019.11.015. Epub 2019 Nov 19. Heart Rhythm. 2020. PMID: 31756529
-
Endocardial pacemaker or defibrillator leads with infected vegetations: a single-center experience and consequences of transvenous extraction.Am Heart J. 2003 Aug;146(2):339-44. doi: 10.1016/S0002-8703(03)00188-1. Am Heart J. 2003. PMID: 12891205
-
Predictors of embolic events in pediatric infective endocarditis.Indian Heart J. 2011 May-Jun;63(3):237-40. Indian Heart J. 2011. PMID: 22734342 Review.
-
Infective Endocarditis: Echocardiographic Imaging and New Imaging Modalities.J Cardiovasc Echogr. 2019 Oct-Dec;29(4):149-155. doi: 10.4103/jcecho.jcecho_53_19. J Cardiovasc Echogr. 2019. PMID: 32089994 Free PMC article. Review.
Cited by
-
Right-Sided Infective Endocarditis 2020: Challenges and Updates in Diagnosis and Treatment.J Am Heart Assoc. 2020 Aug 4;9(15):e017293. doi: 10.1161/JAHA.120.017293. Epub 2020 Jul 23. J Am Heart Assoc. 2020. PMID: 32700630 Free PMC article. Review.
-
Infective Endocarditis among Pediatric Patients with Prosthetic Valves and Cardiac Devices: A Review and Update of Recent Emerging Diagnostic and Management Strategies.J Clin Med. 2023 Jul 27;12(15):4941. doi: 10.3390/jcm12154941. J Clin Med. 2023. PMID: 37568344 Free PMC article. Review.
-
Lead-related infective endocarditis with vegetations: Prevalence and impact of pulmonary embolism in patients undergoing transvenous lead extraction.J Cardiovasc Electrophysiol. 2022 Oct;33(10):2195-2201. doi: 10.1111/jce.15625. Epub 2022 Aug 8. J Cardiovasc Electrophysiol. 2022. PMID: 35842805 Free PMC article.
-
Vacuum-Implemented Removal of Lead Vegetations in Cardiac Device-Related Infective Endocarditis.J Clin Med. 2022 Aug 7;11(15):4600. doi: 10.3390/jcm11154600. J Clin Med. 2022. PMID: 35956217 Free PMC article.
-
Does Age Influence the Preoperative Condition and, Thus, the Outcome in Endocarditis Patients?J Clin Med. 2023 Jan 19;12(3):822. doi: 10.3390/jcm12030822. J Clin Med. 2023. PMID: 36769471 Free PMC article.
References
-
- Santacroce L., D’Agostino D., Charitos I.A., Bottalico L., Ballini A. A short review about electrophysiology and bioimpedance: History and perspectives. Indian J. Public Health Res. Dev. 2018;9:577–591. doi: 10.5958/0976-5506.2018.01521.8. - DOI
-
- Grammes J.A., Schulze C.M., Al-Bataineh M., Yesenosky G.A., Saari C.S., Vrabel M.J., Kutalek S.P. Percutaneous pacemaker and implantable cardioverter-defibrillator lead extraction in 100 patients with intracardiac vegetations defined by transesophageal echocardiogram. J. Am. Coll. Cardiol. 2010;55:886–894. doi: 10.1016/j.jacc.2009.11.034. - DOI - PubMed
LinkOut - more resources
Full Text Sources
