

Role of Citrate in Pathophysiology and Medical Management of Bone Diseases
- PMID: 31731473
- PMCID: PMC6893553
- DOI: 10.3390/nu11112576
Role of Citrate in Pathophysiology and Medical Management of Bone Diseases
Abstract
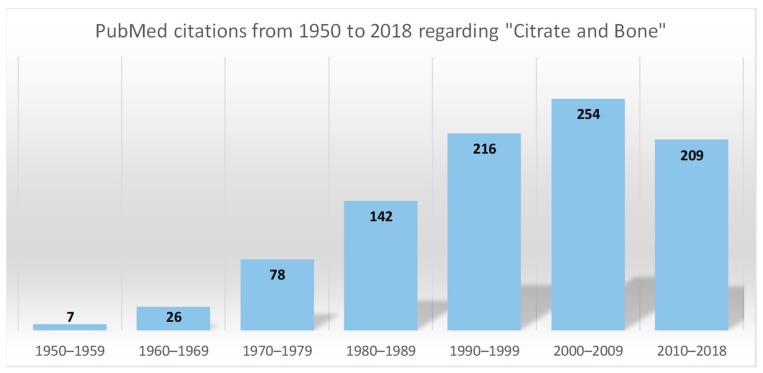
Citrate is an intermediate in the "Tricarboxylic Acid Cycle" and is used by all aerobic organisms to produce usable chemical energy. It is a derivative of citric acid, a weak organic acid which can be introduced with diet since it naturally exists in a variety of fruits and vegetables, and can be consumed as a dietary supplement. The close association between this compound and bone was pointed out for the first time by Dickens in 1941, who showed that approximately 90% of the citrate bulk of the human body resides in mineralised tissues. Since then, the number of published articles has increased exponentially, and considerable progress in understanding how citrate is involved in bone metabolism has been made. This review summarises current knowledge regarding the role of citrate in the pathophysiology and medical management of bone disorders.
Keywords: bone metabolism; bone mineral density; bone remodelling; citrate supplement; kidney diseases; osteopenia; osteoporosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Citrate and mineral metabolism: kidney stones and bone disease.Front Biosci. 2003 Sep 1;8:s1084-106. doi: 10.2741/1119. Front Biosci. 2003. PMID: 12957820 Review.
-
Bone and plasma citrate is reduced in osteoporosis.Bone. 2018 Sep;114:189-197. doi: 10.1016/j.bone.2018.06.014. Epub 2018 Jun 19. Bone. 2018. PMID: 29929041
-
Citrate bridges between mineral platelets in bone.Proc Natl Acad Sci U S A. 2014 Apr 8;111(14):E1354-63. doi: 10.1073/pnas.1315080111. Epub 2014 Mar 24. Proc Natl Acad Sci U S A. 2014. PMID: 24706850 Free PMC article.
-
Dietary treatment of urinary risk factors for renal stone formation. A review of CLU Working Group.Arch Ital Urol Androl. 2015 Jul 7;87(2):105-20. doi: 10.4081/aiua.2015.2.105. Arch Ital Urol Androl. 2015. PMID: 26150027 Review.
-
[Use of citrate in patients with nephrolithiasis].G Ital Nefrol. 2017 Aug 1;34(4):51-60. G Ital Nefrol. 2017. PMID: 28762682 Review. Italian.
Cited by
-
NMR Metabolomics Assessment of Osteogenic Differentiation of Adipose-Tissue-Derived Mesenchymal Stem Cells.J Proteome Res. 2022 Mar 4;21(3):654-670. doi: 10.1021/acs.jproteome.1c00832. Epub 2022 Jan 21. J Proteome Res. 2022. PMID: 35061379 Free PMC article.
-
Fluorescent, Prussian Blue-Based Biocompatible Nanoparticle System for Multimodal Imaging Contrast.Nanomaterials (Basel). 2020 Aug 31;10(9):1732. doi: 10.3390/nano10091732. Nanomaterials (Basel). 2020. PMID: 32878344 Free PMC article.
-
Regional citrate anticoagulation with continuous renal replacement therapy as a cause of hypercalcemia.Arch Osteoporos. 2024 Aug 24;19(1):78. doi: 10.1007/s11657-024-01434-y. Arch Osteoporos. 2024. PMID: 39180669
-
NMR metabolomic modelling of age and lifespan: a multi-cohort analysis.medRxiv [Preprint]. 2023 Nov 8:2023.11.07.23298200. doi: 10.1101/2023.11.07.23298200. medRxiv. 2023. Update in: Aging Cell. 2024 Jul;23(7):e14164. doi: 10.1111/acel.14164. PMID: 37986811 Free PMC article. Updated. Preprint.
-
Calcium Chelidonate: Semi-Synthesis, Crystallography, and Osteoinductive Activity In Vitro and In Vivo.Pharmaceuticals (Basel). 2021 Jun 17;14(6):579. doi: 10.3390/ph14060579. Pharmaceuticals (Basel). 2021. PMID: 34204329 Free PMC article.
References
-
- [(accessed on 4 July 2019)]; Available online: https://www.genome.jp/kegg-bin/show_pathway?map00020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
