

Long-Term Survival after Invasive or Conservative Strategy in Elderly Patients with non-ST-Elevation Myocardial Infarction: A Prospective Cohort Study
- PMID: 31689705
- PMCID: PMC6943809
- DOI: 10.1159/000503442
Long-Term Survival after Invasive or Conservative Strategy in Elderly Patients with non-ST-Elevation Myocardial Infarction: A Prospective Cohort Study
Abstract
Background: The optimal management of elderly patients with non-ST-segment elevation myocardial infarction (NSTEMI) is still discussed. We aimed to study short- and long-term survival in NSTEMI patients ≥75 years managed with an invasive or a conservative strategy.
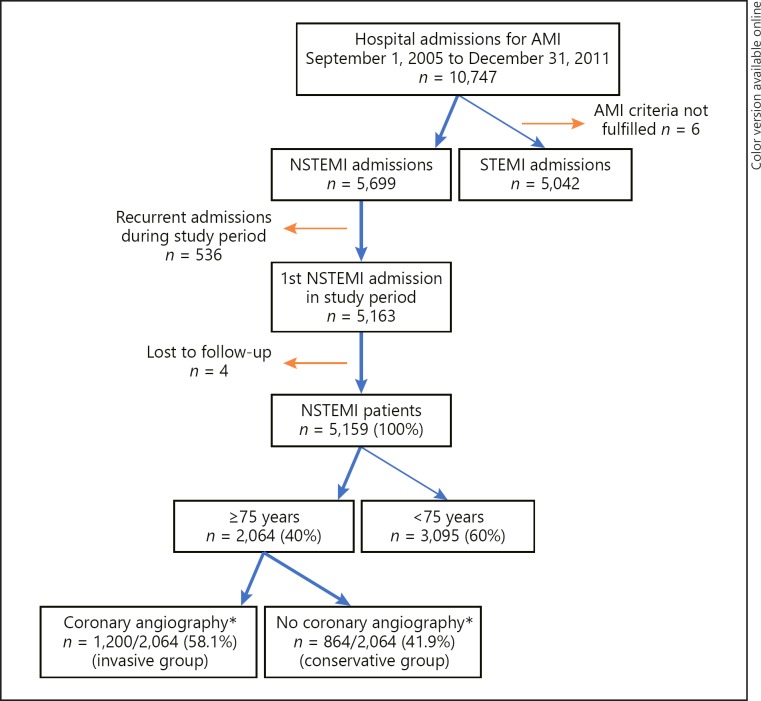
Methods: NSTEMI patients admitted to Oslo University Hospital Ulleval during 2005-2011 were included consecutively in a prospective registry. Vital status until December 31, 2013, was obtained from the Norwegian Cause of Death Registry. Patients ≥75 years were identified, and 30-day and 7-year survival were analyzed. Logistic- and Cox regression was used to estimate OR and hazard ratio (HR) for death in the invasive versus conservative group, adjusting for registered confounders.
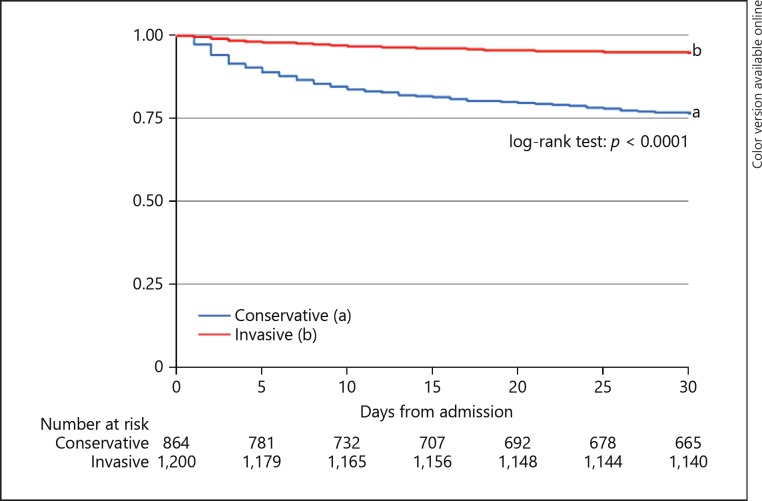
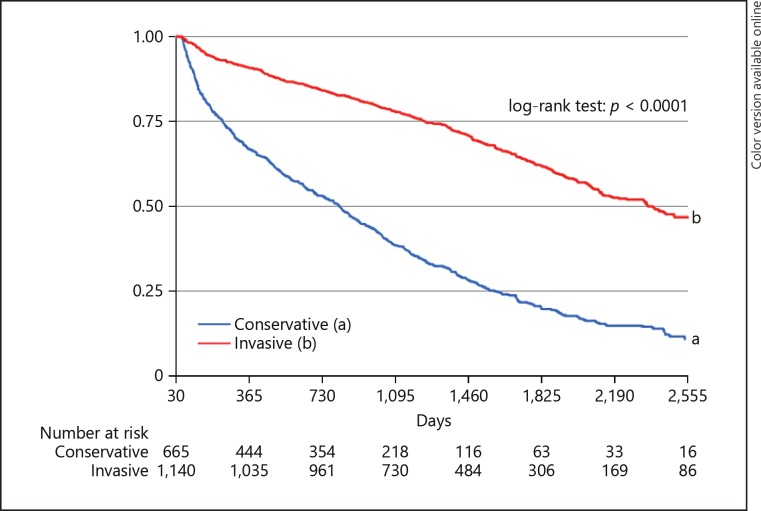
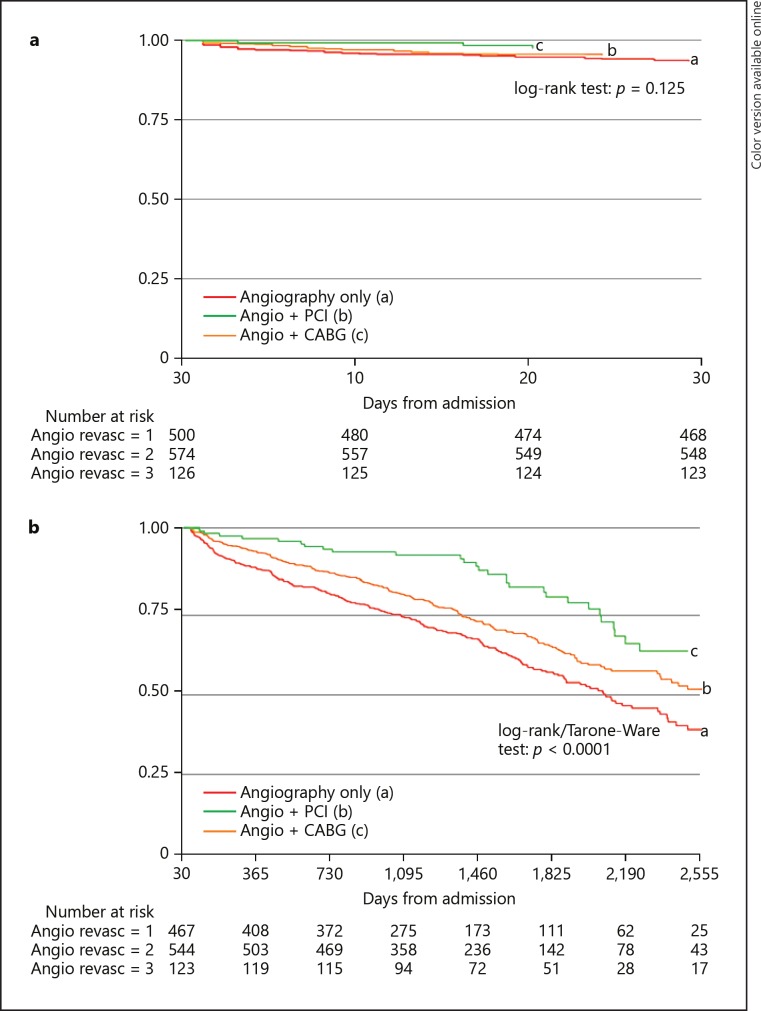
Results: There were 2,064 NSTEMI patients ≥75 years (48.2% women); 1,200 (58.1%) were treated with an invasive strategy, and were younger, more likely to be male and previously revascularized compared to 864 (41.9%) patients treated conservatively (p < 0.0001 for all). Survival at 30-day was 94.9% in the invasive and 76.6% in the conservative group. For 30-day survivors, 7-year survival was 47.4% (95% CI 42.9-51.8) and 11.6% (95% CI 8.3-15.6), respectively. After multivariate adjustment, an invasive strategy was associated with lower long-term risk (adjusted HR [aHR] 0.49 [95% CI 0.41-0.59]). Actual revascularization was associated with lower risk of long-term mortality compared to angiography only (aHRPCI 0.73 [95% CI 0.59-0.90], aHRCABG 0.43 [95% CI 0.28-0.65]).
Conclusion: In this real-life cohort of NSTEMI patients ≥75 years, 30-day survival was 95%, and 7-year survival was 47% with an invasive strategy. Revascularized patients had a superior long-term prognosis. With a conservative strategy, short- and long-term survival was lower, probably due to selection bias and unmeasured confounding.
Keywords: Elderly; Invasive strategy; Long-term survival; Non-ST-segment elevation myocardial infarction.
The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Rationale and design of the DEAR-OLD trial: Randomized evaluation of routinely Deferred versus EARly invasive strategy in elderly patients of 75 years or OLDer with non-ST-elevation myocardial infarction.Am Heart J. 2018 Feb;196:65-73. doi: 10.1016/j.ahj.2017.10.022. Epub 2017 Nov 5. Am Heart J. 2018. PMID: 29421016
-
Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial.JAMA Intern Med. 2023 May 1;183(5):407-415. doi: 10.1001/jamainternmed.2023.0047. JAMA Intern Med. 2023. PMID: 36877502 Free PMC article.
-
Invasive Treatment Strategy for Older Patients with Myocardial Infarction.N Engl J Med. 2024 Nov 7;391(18):1673-1684. doi: 10.1056/NEJMoa2407791. Epub 2024 Sep 1. N Engl J Med. 2024. PMID: 39225274 Clinical Trial.
-
Invasive and antiplatelet treatment of patients with non-ST-segment elevation myocardial infarction: Understanding and addressing the global risk-treatment paradox.Clin Cardiol. 2019 Oct;42(10):1028-1040. doi: 10.1002/clc.23232. Epub 2019 Jul 17. Clin Cardiol. 2019. PMID: 31317575 Free PMC article. Review.
-
Early invasive versus conservative strategies for unstable angina & non-ST-elevation myocardial infarction in the stent era.Cochrane Database Syst Rev. 2006 Jul 19;(3):CD004815. doi: 10.1002/14651858.CD004815.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2010 Mar 17;(3):CD004815. doi: 10.1002/14651858.CD004815.pub3 PMID: 16856061 Updated. Review.
Cited by
-
Invasive Versus Conservative Management of NSTEMI Patients Aged ≥ 75 Years.Arq Bras Cardiol. 2023 May 26;120(6):e20220658. doi: 10.36660/abc.20220658. eCollection 2023. Arq Bras Cardiol. 2023. PMID: 37255135 Free PMC article. English, Portuguese.
-
The role of late reperfusion in ST-segment elevation myocardial infarction: a real-world retrospective cohort study.BMC Cardiovasc Disord. 2020 Apr 28;20(1):207. doi: 10.1186/s12872-020-01479-0. BMC Cardiovasc Disord. 2020. PMID: 32345243 Free PMC article.
-
Non-ST elevation acute coronary syndromes; clinical landscape, management strategy and in-hospital outcomes: an age perspective.Egypt Heart J. 2021 Mar 31;73(1):33. doi: 10.1186/s43044-021-00155-8. Egypt Heart J. 2021. PMID: 33788051 Free PMC article.
-
Conservative versus Invasive Strategy in Elderly Patients with Non-ST-Elevation Myocardial Infarction: Insights from the International POPular Age Registry.J Clin Med. 2023 Aug 22;12(17):5450. doi: 10.3390/jcm12175450. J Clin Med. 2023. PMID: 37685517 Free PMC article.
References
-
- Lagerqvist B, Husted S, Kontny F, Ståhle E, Swahn E, Wallentin L, Fast Revascularisation during InStability in Coronary artery disease (FRISC-II) Investigators 5-year outcomes in the FRISC-II randomised trial of an invasive versus a non-invasive strategy in non-ST-elevation acute coronary syndrome: a follow-up study. Lancet. 2006 Sep;368((9540)):998–1004. - PubMed
-
- Fox KA, Clayton TC, Damman P, Pocock SJ, de Winter RJ, Tijssen JG, et al. FIR Collaboration Long-term outcome of a routine versus selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome a meta-analysis of individual patient data. J Am Coll Cardiol. 2010 Jun;55((22)):2435–45. - PubMed
-
- Damman P, Clayton T, Wallentin L, Lagerqvist B, Fox KA, Hirsch A, et al. Effects of age on long-term outcomes after a routine invasive or selective invasive strategy in patients presenting with non-ST segment elevation acute coronary syndromes: a collaborative analysis of individual data from the FRISC II - ICTUS - RITA-3 (FIR) trials. Heart. 2012 Feb;98((3)):207–13. - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. ESC Scientific Document Group 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016 Jan;37((3)):267–315. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr, Ganiats TG, Holmes DR, Jr, et al. ACC/AHA Task Force Members. Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec;130((25)):2354–94. - PubMed
