

Catecholamine-Secreting Tumors in Pediatric Patients With Cyanotic Congenital Heart Disease
- PMID: 31687640
- PMCID: PMC6821216
- DOI: 10.1210/js.2019-00226
Catecholamine-Secreting Tumors in Pediatric Patients With Cyanotic Congenital Heart Disease
Abstract
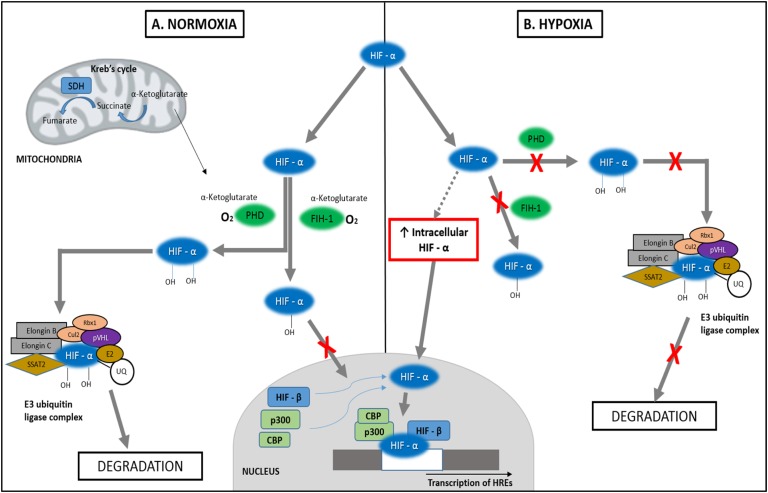
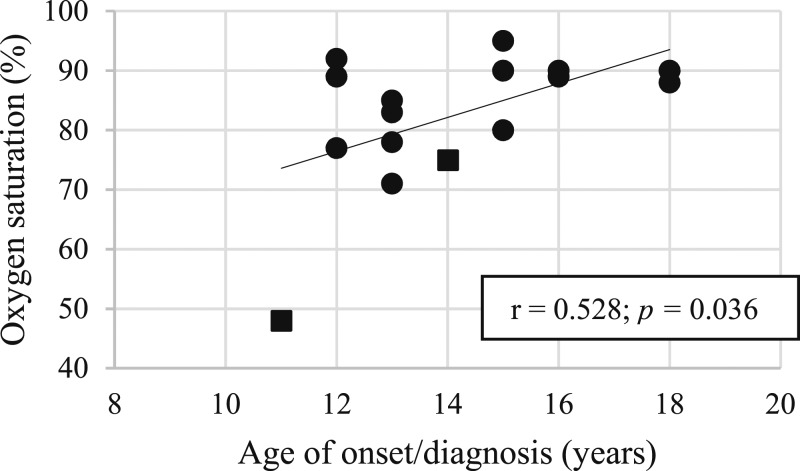
Catecholamine-secreting tumors are rare among the pediatric population but are increasingly being reported in children with sustained hypoxia secondary to cyanotic congenital heart disease (CCHD). With this review, we report the clinical characteristics of these tumors in children with CCHD. The articles included in the present review were identified using PubMed through February 2019. A manual search of the references retrieved from relevant articles was also performed. Pheochromocytomas and paragangliomas (PPGL) in children are commonly associated with high-risk germline or somatic mutations. There is evidently a higher risk of tumorigenesis in children with CCHD as compared with the general pediatric population, even in the absence of susceptible gene mutations. This is due to molecular mechanisms involving the aberrant activation of hypoxia-response elements, likely secondary to sustained hypoxemia, resulting in tumorigenesis. Due to overlapping symptoms with CCHD, the diagnosis of PPGL may be delayed or missed in these patients. We studied all previously reported PPGL cases in children with CCHD and reviewed phenotypic and biochemical features to assess for contributing factors in tumorigenesis. Larger studies are needed to help determine other potential predisposing factors and to establish screening guidelines in this high-risk population. A delay in diagnosis of the PPGL tumors can lead to exacerbation of cardiac failure, and therefore early diagnosis and intervention may provide better outcomes in these patients, necessitating the need for regular surveillance. We recommend routine biochemical screening in patients with sustained hypoxia secondary to CCHD.
Keywords: catecholamine secreting tumors; cyanotic congenital heart disease; hypoxia induced tumorigenesis; paraganglioma; pheochromocytoma.
Copyright © 2019 Endocrine Society.
Figures
Similar articles
-
Genetic Analysis of Pheochromocytoma and Paraganglioma Complicating Cyanotic Congenital Heart Disease.J Clin Endocrinol Metab. 2022 Aug 18;107(9):2545-2555. doi: 10.1210/clinem/dgac362. J Clin Endocrinol Metab. 2022. PMID: 35730597
-
Congenital Cyanotic Heart Disease and the Association with Pheochromocytomas and Paragangliomas.Curr Cardiol Rep. 2023 Nov;25(11):1451-1460. doi: 10.1007/s11886-023-01974-8. Epub 2023 Oct 17. Curr Cardiol Rep. 2023. PMID: 37847359 Review.
-
Comparison of plasma metanephrines in patients with cyanotic and acyanotic congenital heart disease.Endocrine. 2022 Dec;78(3):580-586. doi: 10.1007/s12020-022-03205-6. Epub 2022 Oct 4. Endocrine. 2022. PMID: 36194345
-
Pheochromocytoma and paraganglioma in cyanotic congenital heart disease.J Clin Endocrinol Metab. 2015 Apr;100(4):1325-34. doi: 10.1210/jc.2014-3863. Epub 2015 Jan 12. J Clin Endocrinol Metab. 2015. PMID: 25581599 Free PMC article.
-
Cyanotic congenital heart disease (CCHD): focus on hypoxemia, secondary erythrocytosis, and coagulation alterations.Paediatr Anaesth. 2015 Oct;25(10):981-9. doi: 10.1111/pan.12705. Epub 2015 Jul 17. Paediatr Anaesth. 2015. PMID: 26184479 Review.
Cited by
-
Carney Triad, Carney-Stratakis Syndrome, 3PAS and Other Tumors Due to SDH Deficiency.Front Endocrinol (Lausanne). 2021 May 3;12:680609. doi: 10.3389/fendo.2021.680609. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34012423 Free PMC article. Review.
-
HIF and MYC signaling in adrenal neoplasms of the neural crest: implications for pediatrics.Front Endocrinol (Lausanne). 2023 Jun 8;14:1022192. doi: 10.3389/fendo.2023.1022192. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37361539 Free PMC article. Review.
References
-
- Fishbein L, Leshchiner I, Walter V, Danilova L, Robertson AG, Johnson AR, Lichtenberg TM, Murray BA, Ghayee HK, Else T, Ling S, Jefferys SR, de Cubas AA, Wenz B, Korpershoek E, Amelio AL, Makowski L, Rathmell WK, Gimenez-Roqueplo AP, Giordano TJ, Asa SL, Tischler AS, Pacak K, Nathanson KL, Wilkerson MD; Cancer Genome Atlas Research Network. Comprehensive molecular characterization of pheochromocytoma and paraganglioma. Cancer Cell. 2017;31(2):181–193. - PMC - PubMed
-
- Gimenez-Roqueplo AP, Dahia PL, Robledo M. An update on the genetics of paraganglioma, pheochromocytoma, and associated hereditary syndromes. Horm Metab Res. 2012;44(5):328–333. - PubMed
-
- Wyszyńska T, Cichocka E, Wieteska-Klimczak A, Jobs K, Januszewicz P. A single pediatric center experience with 1025 children with hypertension. Acta Paediatr. 1992;81(3):244–246. - PubMed
-
- Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, Naruse M, Pacak K, Young WF Jr; Endocrine Society. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(6):1915–1942. - PubMed
-
- Omura M, Saito J, Yamaguchi K, Kakuta Y, Nishikawa T. Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens Res. 2004;27(3):193–202. - PubMed
Publication types
LinkOut - more resources
Full Text Sources