

Assessing adherence and cost-benefit of colorectal cancer screening for accountable providers
- PMID: 31656403
- PMCID: PMC6793958
- DOI: 10.1080/08998280.2019.1647702
Assessing adherence and cost-benefit of colorectal cancer screening for accountable providers
Abstract
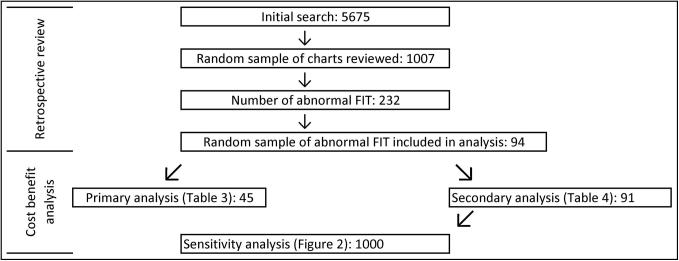
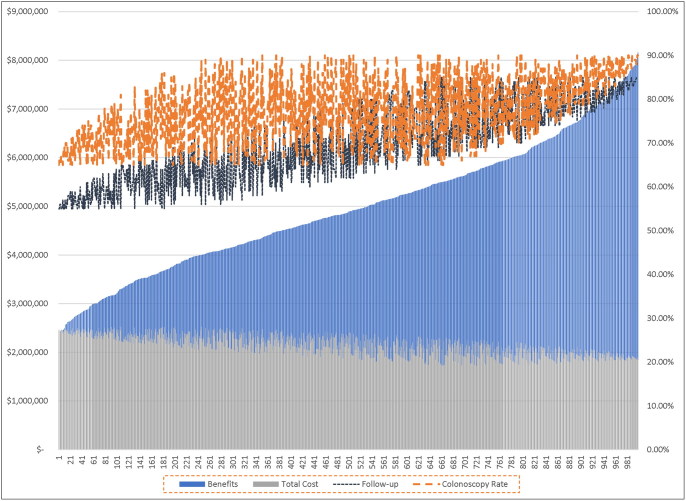
The objective of this study was to assess adherence and costs-benefits of colorectal cancer (CRC) screenings from an accountable care organization/population health perspective. We performed a retrospective review of 94 patients (50-75 years of age) in an integrated safety net system for whom fecal CRC screening was abnormal for the period of June 1, 2014, to June 1, 2016. A cost-benefit model was constructed using Medicare payment rates and a sensitivity analysis. Most patients included in the study (64/94, 68%) received or were offered a colonoscopy. Of those receiving a colonoscopy, 24 of 45 (53%) had an abnormal finding. Total direct medical costs avoided by screening the patient panel was $32,926 but could have exceeded $63,237 had more patients received follow-up colonoscopies. A sensitivity analysis with 1000 patients demonstrated total monetary benefits between $2.2 million and $8.16 million when follow-up and colonoscopy rates were allowed to vary. Although the resulting rates of follow-up were within the range reported in the literature, there is room for improvement, especially considering the monetary benefit that could be used on other diseases. Health systems and payers should work cooperatively to structure payment models to better incentivize CRC screenings.
Keywords: Colorectal cancer screening; cost-benefit model; preventive care.
© 2019 Baylor University Medical Center.
Figures
Similar articles
-
Contrasting Effectiveness and Cost-Effectiveness of Colorectal Cancer Screening Under Commercial Insurance vs. Medicare.Am J Gastroenterol. 2018 Dec;113(12):1836-1847. doi: 10.1038/s41395-018-0106-8. Epub 2018 Jun 15. Am J Gastroenterol. 2018. PMID: 29904156 Free PMC article.
-
Health benefits and cost-effectiveness of a hybrid screening strategy for colorectal cancer.Clin Gastroenterol Hepatol. 2013 Sep;11(9):1158-66. doi: 10.1016/j.cgh.2013.03.013. Epub 2013 Mar 28. Clin Gastroenterol Hepatol. 2013. PMID: 23542330
-
Cost-effectiveness and budget impact analyses of colorectal cancer screenings in a low- and middle-income country: example from Thailand.J Med Econ. 2019 Dec;22(12):1351-1361. doi: 10.1080/13696998.2019.1674065. Epub 2019 Oct 12. J Med Econ. 2019. PMID: 31560247
-
Cost-Effectiveness of DNA Stool Testing to Screen for Colorectal Cancer [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2007 Dec 20. Rockville (MD): Agency for Healthcare Research and Quality (US); 2007 Dec 20. PMID: 25879132 Free Books & Documents. Review.
-
Screening for Colorectal Cancer: An Updated Systematic Review [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Oct. Report No.: 08-05-05124-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Oct. Report No.: 08-05-05124-EF-1. PMID: 20722162 Free Books & Documents. Review.
Cited by
-
Cost-Effectiveness of Colorectal Cancer Genetic Testing.Int J Environ Res Public Health. 2021 Aug 6;18(16):8330. doi: 10.3390/ijerph18168330. Int J Environ Res Public Health. 2021. PMID: 34444091 Free PMC article.
-
Preventing Breast, Cervical, and Colorectal Cancer Deaths: Assessing the Impact of Increased Screening.Prev Chronic Dis. 2020 Oct 8;17:E123. doi: 10.5888/pcd17.200039. Prev Chronic Dis. 2020. PMID: 33034556 Free PMC article.
References
LinkOut - more resources
Full Text Sources