

Determining the clinical significance of co-colonization of vancomycin-resistant enterococci and methicillin-resistant Staphylococcus aureus in the intestinal tracts of patients in intensive care units: a case-control study
- PMID: 31601221
- PMCID: PMC6785887
- DOI: 10.1186/s12941-019-0327-8
Determining the clinical significance of co-colonization of vancomycin-resistant enterococci and methicillin-resistant Staphylococcus aureus in the intestinal tracts of patients in intensive care units: a case-control study
Abstract
Background: The emergence of vancomycin-resistant Staphylococcus aureus (VRSA) has become a global concern for public health. The proximity of vancomycin-resistant enterococcus (VRE) and methicillin-resistant S. aureus (MRSA) is considered to be one of the foremost risk factors for the development of VRSA. This study aimed to determine the incidence, risk factors, and clinical outcomes of intestinal co-colonization with VRE and MRSA.
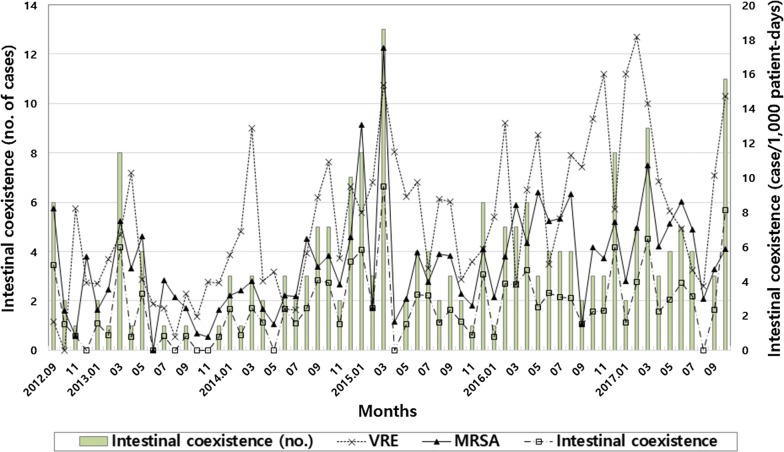
Methods: A case-control study was conducted in 52-bed intensive care units (ICUs) of a university-affiliated hospital from September 2012 to October 2017. Active surveillance using rectal cultures for VRE were conducted at ICU admission and on a weekly basis. Weekly surveillance cultures for detection of rectal MRSA were also conducted in patients with VRE carriage. Patients with intestinal co-colonization of VRE and MRSA were compared with randomly selected control patients with VRE colonization alone (1:1). Vancomycin minimum inhibitory concentrations (MICs) for MRSA isolates were determined by the Etest.
Results: Of the 4679 consecutive patients, 195 cases and 924 controls were detected. The median monthly incidence and duration of intestinal co-colonization with VRE and MRSA were 2.3/1000 patient-days and 7 days, respectively. The frequency of both MRSA infections and mortality attributable to MRSA were higher in the case group than in the control group: 56.9% vs. 44.1% (P = 0.011) and 8.2% vs. 1.0% (P = 0.002), respectively. Independent risk factors for intestinal co-colonization were enteral tube feeding (odds ratio [OR], 2.09; 95% confidence interval [CI] 1.32-3.32), metabolic diseases (OR, 1.75; 95% CI 1.05-2.93), male gender (OR, 1.62; 95% CI 1.06-2.50), and Charlson comorbidity index < 3 (OR, 3.61; 95% CI 1.88-6.94). All MRSA isolates from case patients were susceptible to vancomycin (MIC ≤ 2 mg/L).
Conclusions: Our study indicates that intestinal co-colonization of VRE and MRSA occurs commonly among patients in the ICU with MRSA endemicity, which might be associated with poor clinical outcomes.
Keywords: Active surveillance; Infection control; Methicillin-resistant Staphylococcus aureus; Risk factor; Vancomycin-resistant enterococci.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Predictors of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci co-colonization among nursing facility patients.Am J Infect Control. 2019 Apr;47(4):415-420. doi: 10.1016/j.ajic.2018.09.026. Epub 2018 Nov 28. Am J Infect Control. 2019. PMID: 30502107 Free PMC article.
-
Recovery of both vancomycin-resistant enterococci and methicillin-resistant Staphylococcus aureus from culture of a single clinical specimen from colonized or infected patients.Infect Control Hosp Epidemiol. 2009 Feb;30(2):130-8. doi: 10.1086/593957. Infect Control Hosp Epidemiol. 2009. PMID: 19128183
-
Wounds, functional disability, and indwelling devices are associated with cocolonization by methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci in southeast Michigan.Clin Infect Dis. 2011 Dec;53(12):1215-22. doi: 10.1093/cid/cir733. Clin Infect Dis. 2011. PMID: 22080118 Free PMC article.
-
Natural history of colonization with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE): a systematic review.BMC Infect Dis. 2014 Mar 31;14:177. doi: 10.1186/1471-2334-14-177. BMC Infect Dis. 2014. PMID: 24678646 Free PMC article. Review.
-
Methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococci co-colonization in patients: A meta-analysis.Am J Infect Control. 2020 Aug;48(8):925-932. doi: 10.1016/j.ajic.2019.11.010. Epub 2019 Dec 19. Am J Infect Control. 2020. PMID: 31864808 Review.
Cited by
-
Prevalence and Antibiotic Susceptibility Trends of Selected Enterobacteriaceae, Enterococci, and Candida albicans in the Subgingival Microbiota of German Periodontitis Patients: A Retrospective Surveillance Study.Antibiotics (Basel). 2022 Mar 14;11(3):385. doi: 10.3390/antibiotics11030385. Antibiotics (Basel). 2022. PMID: 35326848 Free PMC article.
-
Lysine Inhibits Hemolytic Activity of Staphylococcus aureus and Its Application in Food Model Contaminated with Staphylococcus aureus.Toxins (Basel). 2022 Dec 9;14(12):867. doi: 10.3390/toxins14120867. Toxins (Basel). 2022. PMID: 36548764 Free PMC article.
-
Bacteriophage endolysin Ply113 as a potent antibacterial agent against polymicrobial biofilms formed by enterococci and Staphylococcus aureus.Front Microbiol. 2023 Dec 12;14:1304932. doi: 10.3389/fmicb.2023.1304932. eCollection 2023. Front Microbiol. 2023. PMID: 38152375 Free PMC article.
-
Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics.Microorganisms. 2023 Jan 6;11(1):149. doi: 10.3390/microorganisms11010149. Microorganisms. 2023. PMID: 36677441 Free PMC article.
-
Total Synthesis of Pargamicin A.Org Lett. 2022 Dec 23;24(50):9285-9289. doi: 10.1021/acs.orglett.2c03861. Epub 2022 Dec 14. Org Lett. 2022. PMID: 36516292 Free PMC article.
References
-
- Kim D, Ahn JY, Lee CH, Jang SJ, Lee H, Yong D, et al. Increasing resistance to extended-spectrum cephalosporins, fluoroquinolone, and carbapenem in gram-negative bacilli and the emergence of carbapenem non-susceptibility in Klebsiella pneumoniae: analysis of Korean Antimicrobial Resistance Monitoring System (KARMS) data from 2013 to 2015. Ann Lab Med. 2017;37:231–239. doi: 10.3343/alm.2017.37.3.231. - DOI - PMC - PubMed
-
- Hawser SP, Bouchillon SK, Hoban DJ, Dowzicky M, Babinchak T. Rising incidence of Staphylococcus aureus with reduced susceptibility to vancomycin and susceptibility to antibiotics: a global analysis 2004–2009. Int J Antimicrob Agents. 2011;37:219–224. doi: 10.1016/j.ijantimicag.2010.10.029. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
