

Chlamydia-induced reactive arthritis diagnosed during gout flares: A case report and cumulative effect of inflammatory cytokines on chronic arthritis
- PMID: 31577714
- PMCID: PMC6783181
- DOI: 10.1097/MD.0000000000017233
Chlamydia-induced reactive arthritis diagnosed during gout flares: A case report and cumulative effect of inflammatory cytokines on chronic arthritis
Abstract
Rationale: The pathology of gouty arthritis and reactive arthritis (ReA) partially overlaps, and both diseases are characterized by the production of inflammatory cytokines associated with the activation of monocytes and macrophages. However, the precise cytokine profile of cases with a coexistence of both diseases is unknown, and there are few reports on the course of treatment in patients with both gouty arthritis and ReA.
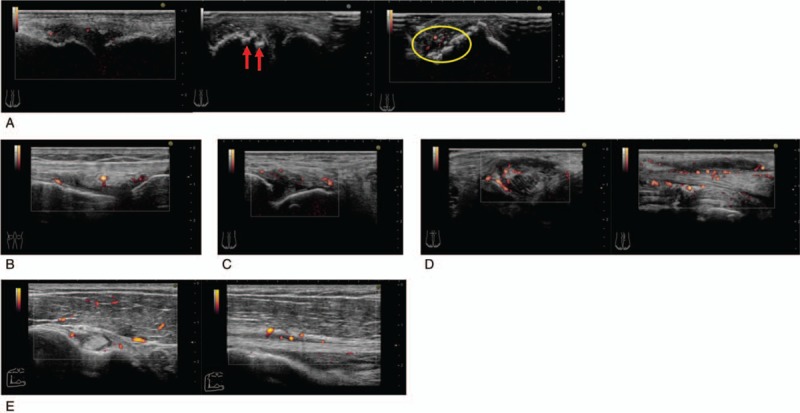
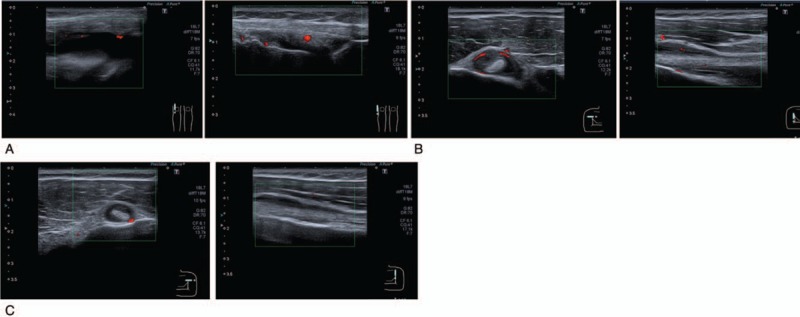
Patient concerns: A 39-year-old man with a recurrent episode of gouty arthritis presented prednisolone-resistant polyarthritis with high level of C-reactive protein (CRP). He had the features of gouty arthritis such as active synovitis of the first manifestation of metatarsophalangeal (MTP) joints and the presence of monosodium urate (MSU) crystals from synovial fluid. But he also had the features of ReA such as the presence of tenosynovitis in the upper limb, the positivity of human leukocyte antigen (HLA)-B27, a history of sexual contact and positive findings of anti-Chlamydia trachomatis-specific IgA and IgG serum antibodies.
Diagnoses: He was diagnosed with HLA-B27 associated Chlamydia-induced ReA accompanied by gout flares.
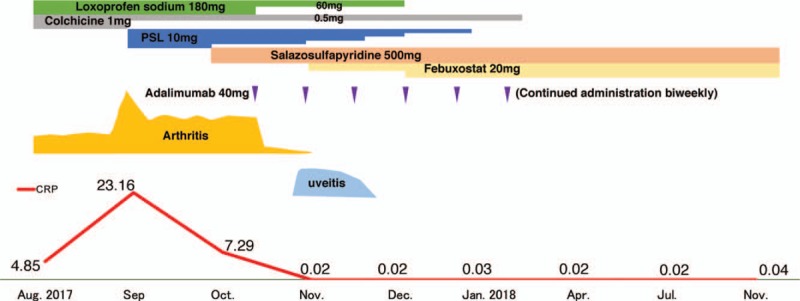
Interventions: He was treated with 180 mg/day of loxoprofen, 1 mg/day of colchicine, and 10 mg/day of prednisolone for gout flares. However, his polyarthritis worsened with an increased level of CRP (23.16 mg/dL). Accordingly, we added 500 mg/day of salazosulfapyridine followed by adalimumab (ADA) 40 mg once every 2 weeks.
Outcomes: After starting ADA, the patient's symptoms and laboratory findings showed rapid improvement and he achieved clinical remission 1 month after initiation of ADA treatment. As of this writing, the patient's clinical remission has been maintained for >1 year.
Lessons: This case suggests that with exacerbation of arthritis during gouty arthritis, coexistence with other pathologies such as peripheral spondyloarthritis should be considered, and early intensive treatment including tumor necrosis factor inhibitors may be necessary.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
[Chlamydia-induced reactive arthritis--HLA-B 27 negative two patients].Ryumachi. 1999 Feb;39(1):11-6. Ryumachi. 1999. PMID: 10332211 Japanese.
-
Plasma adsorption in refractory chronic gouty arthritis flare: A case report.Front Immunol. 2022 Nov 24;13:1045982. doi: 10.3389/fimmu.2022.1045982. eCollection 2022. Front Immunol. 2022. PMID: 36505444 Free PMC article.
-
Use of HLA-B27 tetramers to identify low-frequency antigen-specific T cells in Chlamydia-triggered reactive arthritis.Arthritis Res Ther. 2004;6(6):R521-34. doi: 10.1186/ar1221. Epub 2004 Sep 23. Arthritis Res Ther. 2004. PMID: 15535830 Free PMC article.
-
Reactive arthritis induced by intravesical BCG therapy for bladder cancer: our clinical experience and systematic review of the literature.Autoimmun Rev. 2013 Oct;12(12):1150-9. doi: 10.1016/j.autrev.2013.06.017. Epub 2013 Jun 29. Autoimmun Rev. 2013. PMID: 23816569 Review.
-
[Chlamydia-associated arthritis and enteropathic arthritis--two important spondyloarthritides].Nihon Rinsho Meneki Gakkai Kaishi. 2011;34(3):121-30. doi: 10.2177/jsci.34.121. Nihon Rinsho Meneki Gakkai Kaishi. 2011. PMID: 21720100 Review. Japanese.
Cited by
-
Surgically treated reactive arthritis of the ankle after COVID-19 infection: A case report.J Infect Chemother. 2022 Apr;28(4):587-590. doi: 10.1016/j.jiac.2021.12.028. Epub 2022 Jan 3. J Infect Chemother. 2022. PMID: 35016827 Free PMC article.
-
Approaching Reactive Arthritis Associated With Poor Prognostic Factors: A Case Report and Literature Review.Cureus. 2021 Feb 25;13(2):e13555. doi: 10.7759/cureus.13555. Cureus. 2021. PMID: 33815974 Free PMC article.
-
GSDMD-mediated pyroptosis restrains intracellular Chlamydia trachomatis growth in macrophages.Front Cell Infect Microbiol. 2023 Mar 16;13:1116335. doi: 10.3389/fcimb.2023.1116335. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37009510 Free PMC article.
References
-
- Parathithasan N, Lee WK, Pianta M, et al. Gouty arthropathy: review of clinico-pathologic and imaging features. J Med Imaging Radiat Oncol 2016;60:9–20. - PubMed
-
- Selmi C, Gershwin ME. Diagnosis and classification of reactive arthritis. Autoimmun Rev 2014;13:546–9. - PubMed
-
- Hannu T, Inman R, Granfors K, et al. Reactive arthritis or post-infectious arthritis? Best Pract Res Clin Rheumatol 2006;20:419–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
