

Statin Use in Primary Prevention of Atherosclerotic Cardiovascular Disease According to 5 Major Guidelines for Sensitivity, Specificity, and Number Needed to Treat
- PMID: 31577339
- PMCID: PMC6777225
- DOI: 10.1001/jamacardio.2019.3665
Statin Use in Primary Prevention of Atherosclerotic Cardiovascular Disease According to 5 Major Guidelines for Sensitivity, Specificity, and Number Needed to Treat
Abstract
Importance: Five major guidelines on statin use for primary prevention of atherosclerotic cardiovascular disease (ASCVD) have been published since 2014: the National Institute for Health and Care Excellence (NICE; 2014), US Preventive Services Task Force (USPSTF; 2016), Canadian Cardiovascular Society (CCS; 2016), European Society of Cardiology/European Atherosclerosis Society (ESC/EAS; 2016), and American College of Cardiology/American Heart Association (ACC/AHA; 2018).
Objective: To compare the sensitivity, specificity, and estimated number needed to treat (NNT10) to prevent 1 ASCVD event in 10 years according to statin criteria from the 5 guidelines.
Design, setting, and participants: Population-based contemporary cohort study. Analyses were performed in the Copenhagen General Population Study, with a mean follow-up time of 10.9 years. We included 45 750 individuals aged 40 to 75 years. The participants were enrolled between 2003 and 2009 and were all free of ASCVD at baseline. Data were analyzed between January 1, 2019, and August 4, 2019.
Exposures: Statin treatment according to guideline criteria. We assumed a 25% relative reduction of ASCVD events per 38 mg/dL (to convert to millimoles per liter, multiply by 0.0259) reduction in low-density lipoprotein cholesterol.
Main outcomes and measures: Sensitivity and specificity for ASCVD events and the NNT10 to prevent 1 ASCVD event according to guideline criteria.
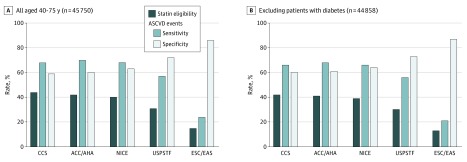
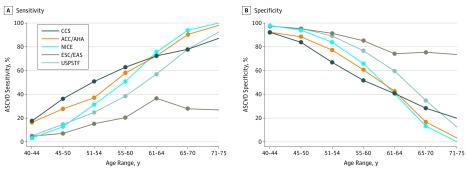
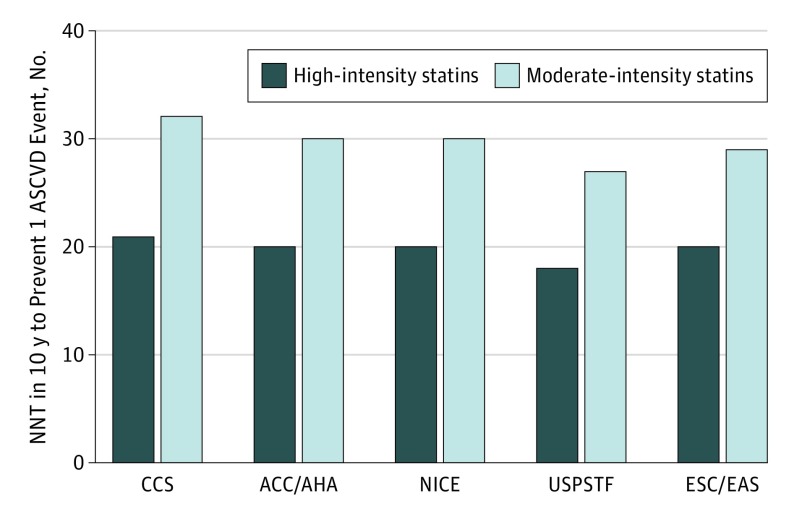
Results: Median age at baseline examination was 56 years, and 43% of participants were men (n = 19 870 of 45 750). During follow-up, we observed 4156 ASCVD events. Overall, 44% of individuals in Copenhagen General Population Study were statin eligible with CCS (n = 19 953 of 45 750), 42% with ACC/AHA (n = 19 400 of 45 750), 40% with NICE (n = 19 400 of 45 750), 31% with USPSTF (n = 13 966 of 45 750), and 15% with ESC/EAS (n = 6870 of 45 750). Sensitivity and specificity for ASCVD events were 68% (n = 2815 of 4156) and 59% (n = 24 456 of 41 594) for CCS, 70% (n = 2889 of 4156) and 60% (n = 25 083 of 41 594) for ACC/AHA, 68% (n = 2815 of 4156) and 63% (n = 26 213 of 41 594) for NICE, 57% (n = 2377 of 4156) and 72% (n = 30 005 of 41 594) for USPSTF, and 24% (n = 1001 of 4156) and 86% (n = 35 725 of 41 594) for ESC/EAS. The NNT10 to prevent 1 ASCVD using moderate-intensity and high-intensity statin therapy, respectively, was 32 and 21 for CCS criteria, 30 and 20 for ACC/AHA criteria, 30 and 20 for NICE criteria, 27 and 18 for USPSTF criteria, and 29 and 20 for ESC/EAS criteria.
Conclusions and relevance: With similar NNT10 to prevent 1 event, the CCS, ACC/AHA, and NICE guidelines correctly assign statin therapy to many more of the individuals who later develop ASCVD compared with the USPSTF and ESC/EAS guidelines. Our results therefore suggest that the CCS, ACC/AHA, or NICE guidelines may be preferred for primary prevention.
Conflict of interest statement
Figures
Similar articles
-
ACC/AHA guidelines superior to ESC/EAS guidelines for primary prevention with statins in non-diabetic Europeans: the Copenhagen General Population Study.Eur Heart J. 2017 Feb 21;38(8):586-594. doi: 10.1093/eurheartj/ehw426. Eur Heart J. 2017. PMID: 28363217 Free PMC article.
-
Comparison of Five Major Guidelines for Statin Use in Primary Prevention in a Contemporary General Population.Ann Intern Med. 2018 Jan 16;168(2):85-92. doi: 10.7326/M17-0681. Epub 2018 Jan 2. Ann Intern Med. 2018. PMID: 29297004
-
Statin Eligibility for Primary Prevention of Cardiovascular Disease According to 2021 European Prevention Guidelines Compared With Other International Guidelines.JAMA Cardiol. 2022 Aug 1;7(8):836-843. doi: 10.1001/jamacardio.2022.1876. JAMA Cardiol. 2022. PMID: 35793078 Free PMC article.
-
Hyperlipidemia: Drugs for Cardiovascular Risk Reduction in Adults.Am Fam Physician. 2017 Jan 15;95(2):78-87. Am Fam Physician. 2017. PMID: 28084704 Review.
-
Major Global Coronary Artery Calcium Guidelines.JACC Cardiovasc Imaging. 2023 Jan;16(1):98-117. doi: 10.1016/j.jcmg.2022.06.018. Epub 2022 Sep 14. JACC Cardiovasc Imaging. 2023. PMID: 36599573 Review.
Cited by
-
Lipid-lowering therapy for primary prevention of premature atherosclerotic coronary artery disease: Eligibility, utilization, target achievement, and predictors of initiation.Am J Prev Cardiol. 2020 Jul 17;2:100036. doi: 10.1016/j.ajpc.2020.100036. eCollection 2020 Jun. Am J Prev Cardiol. 2020. PMID: 34327459 Free PMC article.
-
Effectiveness of glucose-lowering medications on cardiovascular outcomes in patients with type 2 diabetes at moderate cardiovascular risk.Nat Cardiovasc Res. 2024 Apr;3(4):431-440. doi: 10.1038/s44161-024-00453-9. Epub 2024 Apr 3. Nat Cardiovasc Res. 2024. PMID: 38846711 Free PMC article.
-
Uptake of Statin Guidelines to Prevent and Treat Cardiovascular Disease.J Am Board Fam Med. 2021 Jan-Feb;34(1):113-122. doi: 10.3122/jabfm.2021.01.200292. J Am Board Fam Med. 2021. PMID: 33452089 Free PMC article.
-
Metabolic Syndrome in an Aging Society - Role of Oxidant-Antioxidant Imbalance and Inflammation Markers in Disentangling Atherosclerosis.Clin Interv Aging. 2021 Jun 9;16:1057-1070. doi: 10.2147/CIA.S306982. eCollection 2021. Clin Interv Aging. 2021. PMID: 34135578 Free PMC article.
-
Effects of a Secondary Prevention Combination Therapy with beta-Blocker and Statin on Major Adverse Cardiovascular Events in Acute Coronary Syndrome Patients.Med Sci Monit. 2020 Aug 18;26:e925114. doi: 10.12659/MSM.925114. Med Sci Monit. 2020. PMID: 32808600 Free PMC article.
References
-
- National Clinical Guideline Centre. National Institute for Health and Care Excellence (NICE) clinical guideline CG181: lipid modification, cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. https://www.nice.org.uk/guidance/cg181. Published July 2014. Accessed August 28, 2019. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, et al. ; ESC Scientific Document Group . 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315-2381. doi:10.1093/eurheartj/ehw106 - DOI - PMC - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, et al. . AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73(24):3168. doi:10.1016/j.jacc.2018.11.002 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
